PIQRAY Tablet Ref.[9952] Active ingredients: Alpelisib
Source: FDA, National Drug Code (US) Revision Year: 2020
12.1. Mechanism of Action
Alpelisib is an inhibitor of phosphatidylinositol-3-kinase (PI3K) with inhibitory activity predominantly against PI3Kα. Gain-of-function mutations in the gene encoding the catalytic α-subunit of PI3K (PIK3CA) lead to activation of PI3Kα and Akt-signaling, cellular transformation and the generation of tumors in in vitro and in vivo models.
In breast cancer cell lines, alpelisib inhibited the phosphorylation of PI3K downstream targets, including Akt and showed activity in cell lines harboring a PIK3CA mutation. In vivo, alpelisib inhibited the PI3K/Akt signaling pathway and reduced tumor growth in xenograft models, including models of breast cancer.
PI3K inhibition by alpelisib treatment has been shown to induce an increase in estrogen receptor (ER) transcription in breast cancer cells. The combination of alpelisib and fulvestrant demonstrated increased anti-tumor activity compared to either treatment alone in xenograft models derived from ER-positive, PIK3CA mutated breast cancer cell lines.
12.2. Pharmacodynamics
Cardiac Electrophysiology
Serial ECGs were collected following a single dose and at steady-state to evaluate the effect of alpelisib on the QTcF interval in patients with advanced cancer. An analysis of clinical ECG data demonstrates the absence of a large effect (i.e., > 20 ms) on QTcF prolongation at the recommended 300 mg dose with or without fulvestrant.
12.3. Pharmacokinetics
The pharmacokinetics of alpelisib has been studied in healthy subjects and adult patients with solid tumors. Steady-state alpelisib maximum plasma concentration (Cmax) and AUC increased proportionally over the dose range of 30 mg to 450 mg (0.1 to 1.5 times the approved recommended dosage) under fed conditions. The mean accumulation of alpelisib is 1.3 to 1.5 and steady-state plasma concentrations are reached within 3 days following daily dosage. In adult patients who received PIQRAY 300 mg once daily in the SOLAR-1 trial, population approach derived mean steady-state alpelisib [coefficient of variation (CV%)] for Cmax was 2480 (23%) ng/mL and AUC0-24hr was 33224 (21%) ng*h/mL.
Absorption
The median time to reach peak plasma concentration (Tmax) ranged between 2.0 to 4.0 hours.
Effect of food
A high-fat high-calorie meal (985 calories with 58.1 g of fat) increased alpelisib AUC by 73% and Cmax by 84%, and a low-fat low-calorie meal (334 calories with 8.7 g of fat) increased alpelisib AUC by 77% and Cmax by 145% following a single dose of PIQRAY. No clinically significant differences in alpelisib AUC were observed between low-fat low-calorie and high-fat high-calorie meals.
Distribution
The mean (% CV) apparent volume of distribution of alpelisib at steady-state is predicted to be 114 L (46%). Protein binding of alpelisib is 89% and is independent of concentration.
Elimination
The half-life of alpelisib is predicted to be 8 to 9 hours. The mean (% CV) clearance of alpelisib is predicted to be 9.2 L/hr (21%) under fed conditions.
Metabolism
Alpelisib is primarily metabolized by chemical and enzymatic hydrolysis to form its metabolite BZG791 and to a lesser extent by CYP3A4, in vitro.
Excretion
Following a single oral dose of 400 mg radiolabeled alpelisib under fasted condition, 81% of the administered dose was recovered in feces (36% unchanged, 32% BZG791) and 14% (2% unchanged, 7.1% BZG791) in urine. CYP3A4-mediated metabolites (12%) and glucuronides amounted to approximately 15% of the dose.
Specific Populations
No clinically significant differences in the pharmacokinetics of alpelisib were predicted based on age (21 to 87 years), sex, race/ethnicity (Japanese or Caucasian), body weight (37 to 181 kg), mild to moderate renal impairment (CLcr 30 to < 90 mL/min based on the Cockcroft-Gault formula), or mild to severe hepatic impairment (Child-Pugh Class A, B, and C). The effect of severe renal impairment (CLcr < 30 mL/min) on the pharmacokinetics of alpelisib is unknown.
Drug Interaction Studies
Clinical Studies
Acid Reducing Agents: PIQRAY can be coadministered with acid reducing agents, since PIQRAY should be taken with food. Food exhibited a more pronounced effect on the solubility of alpelisib than the effect of gastric pH value.
Coadministration of the H2 receptor antagonist ranitidine in combination with a single 300 mg oral dose of alpelisib decreased the absorption and overall exposure of alpelisib. In the presence of a low-fat low-calorie meal, AUC was decreased on average by 21% and Cmax by 36% with ranitidine. Under the fasted state, AUC was decreased on average by 30% and Cmax by 51% with ranitidine.
CYP3A4 Substrates: No clinically significant differences in pharmacokinetics of everolimus (a substrate of CYP3A4 and P-gp) were observed when coadministered with alpelisib.
In Vitro Studies
Effect of Alpelisib on CYP Enzymes: Alpelisib inhibits CYP3A4 in a time-dependent manner and induces CYP2B6, CYP2C9 and CYP3A4.
Effect of Transporter on Alpelisib: Alpelisib is a substrate of BCRP.
Effect of Alpelisib on Transporters: Alpelisib is an inhibitor of P-gp. Alpelisib has a low potential to inhibit BCRP, MRP2, BSEP, OATP1B1, OATP1B3, OCT1, OAT1, OAT3, OCT2, MATE1, and MATE2K at clinically relevant concentrations.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not been conducted with alpelisib.
Alpelisib was not mutagenic in an in vitro bacterial reverse mutation (Ames) assay, or aneugenic or clastogenic in human cell micronucleus and chromosome aberration tests in vitro. Alpelisib was not genotoxic in an in vivo rat micronucleus test.
Fertility studies in animals have not been conducted. In repeated-dose toxicity studies up to 13 weeks duration, adverse effects were observed in reproductive organs, including vaginal atrophy and estrous cycle variations in rats at doses ≥ 6 mg/kg/day (approximately 0.6 times the exposure in humans at the recommended dose of 300 mg/day based on AUC), and prostate atrophy in dogs at doses ≥ 15 mg/kg/day (approximately 2.6 times the exposure in humans at the recommended dose of 300 mg/day based on AUC).
14. Clinical Studies
SOLAR-1 (NCT02437318) was a randomized, double-blind, placebo-controlled trial of PIQRAY plus fulvestrant versus placebo plus fulvestrant in 572 patients with HR-positive, HER2-negative, advanced or metastatic breast cancer whose disease had progressed or recurred on or after an aromatase inhibitor-based treatment (with or without CDK4/6 combination). Patients were excluded if they had inflammatory breast cancer, diabetes mellitus Type 1 or uncontrolled Type 2, or pneumonitis. Randomization was stratified by presence of lung and/or liver metastasis and previous treatment with CDK4/6 inhibitor(s). Overall, 60% of enrolled patients had tumors with one or more PIK3CA mutations in tissue, 50% had liver/lung metastases, and 6% had previously been treated with a CDK4/6 inhibitor.
There were 341 patients enrolled by tumor tissue in the cohort with a PIK3CA mutation and 231 enrolled in the cohort without a PIK3CA mutation. Of the 341 patients in the cohort with a PIK3CA mutation, 336 (99%) patients had one or more PIK3CA mutations confirmed in tumor tissue using the FDA-approved therascreen PIK3CA RGQ PCR Kit. Out of the 336 patients with PIK3CA mutations confirmed in tumor tissue, 19 patients had no plasma specimen available for testing with the FDA-approved therascreen PIK3CA RGQ PCR Kit. Of the remaining 317 patients with PIK3CA mutations confirmed in tumor tissue, 177 patients (56%) had PIK3CA mutations identified in plasma specimen, and 140 patients (44%) did not have PIK3CA mutations identified in plasma specimen.
Patients received either PIQRAY (300 mg) or placebo orally once daily on a continuous basis, plus fulvestrant (500 mg) administered intramuscularly on Cycle 1, Days 1 and 15, and then on Day 1 of every 28-day cycle. Patients received treatment until radiographic disease progression or unacceptable toxicity. Tumor assessments were performed every 8 weeks for the first 18 months and every 12 weeks thereafter.
The median age of patients was 63 years (range, 25 to 92). Most patients were women (99.8%) and most patients were white (66%), followed by Asian (22%), Other/Unknown (10%), black or African American (1.4%), and American Indian or Alaskan Native (0.9%). Baseline ECOG performance status was 0 (68%) or 1 (32%).
Patient demographics for those with PIK3CA-mutated tumors were generally representative of the broader study population. The median duration of exposure to PIQRAY plus fulvestrant was 8.2 months with 59% of patients exposed for > 6 months.
The majority of patients (98%) received prior hormonal therapy as the last treatment (48% metastatic setting, 52% adjuvant setting). Primary endocrine resistance, defined as relapsed within 24 months on adjuvant endocrine therapy or progression within 6 months on endocrine therapy for advanced disease, was observed in 13% of patients and secondary endocrine resistance, defined as relapsed after 24 months on adjuvant endocrine therapy, relapsed within 12 months of the end of adjuvant endocrine therapy, or progression after 6 months on endocrine therapy for advanced disease, was observed in 72% of patients.
The major efficacy outcome was investigator-assessed progression-free survival (PFS) in the cohort with a PIK3CA mutation per Response Evaluation Criteria in Solid Tumors (RECIST) v1.1. Additional efficacy outcome measures were overall response rate (ORR) and overall survival (OS) in the cohort with a PIK3CA mutation.
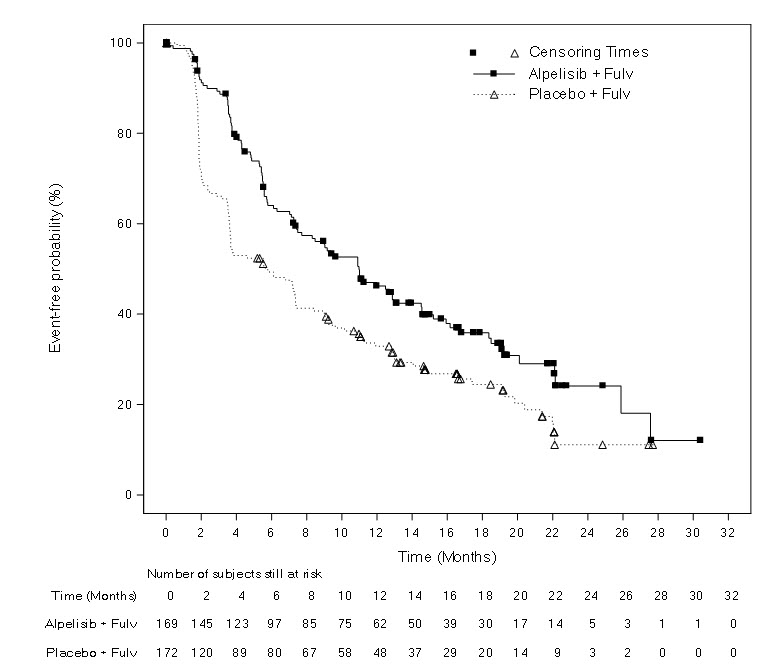
Efficacy results for the cohort with a PIK3CA mutation in tumor tissue are presented in Table 8 and Figure 1. PFS results for the cohort with a PIK3CA mutation by investigator assessment were supported by consistent results from a blinded independent review committee (BIRC) assessment. Consistent results were seen in patients with tissue or plasma PIK3CA mutations. At the time of final PFS analysis, 27% (92/341) of patients had died, and overall survival follow-up was immature.
No PFS benefit was observed in patients whose tumors did not have a PIK3CA tissue mutation (HR = 0.85; 95% CI: 0.58, 1.25).
Table 8: Efficacy Results in SOLAR-1 (Per Investigator Assessment of Patients with a PIK3CA Tumor Mutation)
| PIQRAY plus fulvestrant | Placebo plus fulvestrant | |
|---|---|---|
| Progression-free survival | N = 169 | N = 172 |
| Number of PFS events - n(%) | 103 (61) | 129 (75) |
| Median PFS months (95% CI) | 11.0 (7.5, 14.5) | 5.7 (3.7, 7.4) |
| Hazard ratio (95% CI) | 0.65 (0.50, 0.85) | |
| p-value1 | 0.0013 | |
| Overall Response Rate | N = 126 | N = 136 |
| ORR2 (95% CI) | 35.7 (27.4, 44.7) | 16.2 (10.4, 23.5) |
1Both log-rank test and Cox proportional hazards model are stratified by prior CDK4/6 inhibitor usage and presence of lung/liver metastases. P-value was compared to prespecified Haybittle-Peto stopping boundary (two-sided p ≤ 0.0398).
2ORR = percentage of patients with confirmed Complete Response or Partial Response with measurable disease at baseline.
Figure 1. Progression Free Survival in SOLAR-1 (Per Investigator Assessment of Patients with a PIK3CA Tumor Mutation):
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.