PRAVACHOL Tablet Ref.[10601] Active ingredients: Pravastatin
Source: FDA, National Drug Code (US) Revision Year: 2020
12.1. Mechanism of Action
Pravastatin is a reversible inhibitor of 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase, the enzyme that catalyzes the conversion of HMG-CoA to mevalonate, an early and rate limiting step in the biosynthetic pathway for cholesterol. In addition, pravastatin reduces VLDL and TG and increases HDL-C.
12.3. Pharmacokinetics
General
Absorption
PRAVACHOL is administered orally in the active form. In studies in man, peak plasma pravastatin concentrations occurred 1 to 1.5 hours upon oral administration. Based on urinary recovery of total radiolabeled drug, the average oral absorption of pravastatin is 34% and absolute bioavailability is 17%. While the presence of food in the gastrointestinal tract reduces systemic bioavailability, the lipid-lowering effects of the drug are similar whether taken with or 1 hour prior to meals.
Pravastatin plasma concentrations, including area under the concentration-time curve (AUC), Cmax, and steady-state minimum (Cmin), are directly proportional to administered dose. Systemic bioavailability of pravastatin administered following a bedtime dose was decreased 60% compared to that following an AM dose. Despite this decrease in systemic bioavailability, the efficacy of pravastatin administered once daily in the evening, although not statistically significant, was marginally more effective than that after a morning dose.
The coefficient of variation (CV), based on between-subject variability, was 50% to 60% for AUC. The geometric means of pravastatin Cmax and AUC following a 20 mg dose in the fasted state were 26.5 ng/mL and 59.8 ng*hr/mL, respectively.
Steady-state AUCs, Cmax, and Cmin plasma concentrations showed no evidence of pravastatin accumulation following once or twice daily administration of PRAVACHOL tablets.
Distribution
Approximately 50% of the circulating drug is bound to plasma proteins.
Metabolism
The major biotransformation pathways for pravastatin are: (a) isomerization to 6-epi pravastatin and the 3α-hydroxyisomer of pravastatin (SQ 31,906) and (b) enzymatic ring hydroxylation to SQ 31,945. The 3α-hydroxyisomeric metabolite (SQ 31,906) has 1/10 to 1/40 the HMG-CoA reductase inhibitory activity of the parent compound. Pravastatin undergoes extensive first-pass extraction in the liver (extraction ratio 0.66).
Excretion
Approximately 20% of a radiolabeled oral dose is excreted in urine and 70% in the feces. After intravenous administration of radiolabeled pravastatin to normal volunteers, approximately 47% of total body clearance was via renal excretion and 53% by non-renal routes (i.e., biliary excretion and biotransformation).
Following single dose oral administration of 14C-pravastatin, the radioactive elimination t½ for pravastatin is 1.8 hours in humans.
Specific Populations
Renal Impairment
A single 20 mg oral dose of pravastatin was administered to 24 patients with varying degrees of renal impairment (as determined by creatinine clearance). No effect was observed on the pharmacokinetics of pravastatin or its 3α-hydroxy isomeric metabolite (SQ 31,906). Compared to healthy subjects with normal renal function, patients with severe renal impairment had 69% and 37% higher mean AUC and Cmax values, respectively, and a 0.61 hour shorter t½ for the inactive enzymatic ring hydroxylation metabolite (SQ 31,945).
Hepatic Impairment
In a study comparing the kinetics of pravastatin in patients with biopsy confirmed cirrhosis (N=7) and normal subjects (N=7), the mean AUC varied 18-fold in cirrhotic patients and 5-fold in healthy subjects. Similarly, the peak pravastatin values varied 47-fold for cirrhotic patients compared to 6-fold for healthy subjects. [See Warnings and Precautions (5.3)].
Geriatric
In a single oral dose study using pravastatin 20 mg, the mean AUC for pravastatin was approximately 27% greater and the mean cumulative urinary excretion (CUE) approximately 19% lower in elderly men (65-75 years old) compared with younger men (19-31 years old). In a similar study conducted in women, the mean AUC for pravastatin was approximately 46% higher and the mean CUE approximately 18% lower in elderly women (65-78 years old) compared with younger women (18-38 years old). In both studies, Cmax, Tmax, and t½ values were similar in older and younger subjects. [See Use in Specific Populations (8.5)].
Pediatric
After 2 weeks of once-daily 20 mg oral pravastatin administration, the geometric means of AUC were 80.7 (CV 44%) and 44.8 (CV 89%) ng*hr/mL for children (8-11 years, N=14) and adolescents (12-16 years, N=10), respectively. The corresponding values for Cmax were 42.4 (CV 54%) and 18.6 ng/mL (CV 100%) for children and adolescents, respectively. No conclusion can be made based on these findings due to the small number of samples and large variability. [See Use in Specific Populations (8.4)].
Drug-Drug Interactions
Table 3. Effect of Coadministered Drugs on the Pharmacokinetics of Pravastatin:
| Pravastatin | |||
|---|---|---|---|
| Coadministered Drug and Dosing Regimen | Dose (mg) | Change in AUC | Change in Cmax |
| Cyclosporine 5 mg/kg single dose | 40 mg single dose | ↑282% | ↑327% |
| Clarithromycin 500 mg BID for 9 days | 40 mg OD for 8 days | ↑110% | ↑128% |
| Boceprevir 800 mg TID for 6 days | 40 mg single dose | ↑63% | ↑49% |
| Darunavir 600 mg BID/Ritonavir 100 mg BID for 7 days | 40 mg single dose | ↑81% | ↑63% |
| Colestipol 10 g single dose | 20 mg single dose | ↓47% | ↓53% |
| Cholestyramine 4 g single dose Administered simultaneously Administered 1 hour prior to cholestyramine Administered 4 hours after cholestyramine | 20 mg single dose | ↓40% ↑12% ↓12% | ↓39% ↑30% ↓6.8% |
| Cholestyramine 24 g OD for 4 weeks | 20 mg BID for 8 weeks 5 mg BID for 8 weeks 10 mg BID for 8 weeks | ↓51% ↓38% ↓18% | ↑4.9% ↑23% ↓33% |
| Fluconazole 200 mg IV for 6 days 200 mg PO for 6 days | 20 mg PO+10 mg IV 20 mg PO+10 mg IV | ↓34% ↓16% | ↓33% ↓16% |
| Kaletra 400 mg/100 mg BID for 14 days | 20 mg OD for 4 days | ↑33% | ↑26% |
| Verapamil IR 120 mg for 1 day and Verapamil ER 480 mg for 3 days | 40 mg single dose | ↑31% | ↑42% |
| Cimetidine 300 mg QID for 3 days | 20 mg single dose | ↑30% | ↑9.8% |
| Antacids 15 mL QID for 3 days | 20 mg single dose | ↓28% | ↓24% |
| Digoxin 0.2 mg OD for 9 days | 20 mg OD for 9 days | ↑23% | ↑26% |
| Probucol 500 mg single dose | 20 mg single dose | ↑14% | ↑24% |
| Warfarin 5 mg OD for 6 days | 20 mg BID for 6 days | ↓13% | ↑6.7% |
| Itraconazole 200 mg OD for 30 days | 40 mg OD for 30 days | ↑11% (compared to Day 1) | ↑17% (compared to Day 1) |
| Gemfibrozil 600 mg single dose | 20 mg single dose | ↓7.0% | ↓20% |
| Aspirin 324 mg single dose | 20 mg single dose | ↑4.7% | ↑8.9% |
| Niacin 1 g single dose | 20 mg single dose | ↓3.6% | ↓8.2% |
| Diltiazem | 20 mg single dose | ↑2.7% | ↑30% |
| Grapefruit juice | 40 mg single dose | ↓1.8% | ↑3.7% |
BID = twice daily; OD = once daily; QID = four times daily
Table 4. Effect of Pravastatin on the Pharmacokinetics of Coadministered Drugs:
| Pravastatin Dosing Regimen | Name and Dose | Change in AUC | Change in Cmax |
|---|---|---|---|
| 20 mg BID for 6 days | Warfarin 5 mg OD for 6 days Change in mean prothrombin time | ↑17% ↑0.4 sec | ↑15% |
| 20 mg OD for 9 days | Digoxin 0.2 mg OD for 9 days | ↑4.6% | ↑5.3% |
| 20 mg BID for 4 weeks 10 mg BID for 4 weeks 5 mg BID for 4 weeks | Antipyrine 1.2 g single dose | ↑3.0% ↑1.6% ↑ Less than 1% | Not Reported |
| 20 mg OD for 4 days | Kaletra 400 mg/100 mg BID for 14 days | No change | No change |
BID = twice daily; OD = once daily
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
In a 2-year study in rats fed pravastatin at doses of 10, 30, or 100 mg/kg body weight, there was an increased incidence of hepatocellular carcinomas in males at the highest dose (p<0.01). These effects in rats were observed at approximately 12 times the human dose (HD) of 80 mg based on body surface area (mg/m 2) and at approximately 4 times the HD, based on AUC.
In a 2-year study in mice fed pravastatin at doses of 250 and 500 mg/kg/day, there was an increased incidence of hepatocellular carcinomas in males and females at both 250 and 500 mg/kg/day (p<0.0001). At these doses, lung adenomas in females were increased (p=0.013). These effects in mice were observed at approximately 15 times (250 mg/kg/day) and 23 times (500 mg/kg/day) the HD of 80 mg, based on AUC. In another 2-year study in mice with doses up to 100 mg/kg/day (producing drug exposures approximately 2 times the HD of 80 mg, based on AUC), there were no drug-induced tumors.
No evidence of mutagenicity was observed in vitro, with or without rat-liver metabolic activation, in the following studies: microbial mutagen tests, using mutant strains of Salmonella typhimurium or Escherichia coli; a forward mutation assay in L5178Y TK +/− mouse lymphoma cells; a chromosomal aberration test in hamster cells; and a gene conversion assay using Saccharomyces cerevisiae. In addition, there was no evidence of mutagenicity in either a dominant lethal test in mice or a micronucleus test in mice.
In a fertility study in adult rats with daily doses up to 500 mg/kg, pravastatin did not produce any adverse effects on fertility or general reproductive performance.
13.2. Animal Toxicology and/or Pharmacology
CNS Toxicity
CNS vascular lesions, characterized by perivascular hemorrhage and edema and mononuclear cell infiltration of perivascular spaces, were seen in dogs treated with pravastatin at a dose of 25 mg/kg/day. These effects in dogs were observed at approximately 59 times the HD of 80 mg/day, based on AUC. Similar CNS vascular lesions have been observed with several other drugs in this class.
A chemically similar drug in this class produced optic nerve degeneration (Wallerian degeneration of retinogeniculate fibers) in clinically normal dogs in a dose-dependent fashion starting at 60 mg/kg/day, a dose that produced mean plasma drug levels about 30 times higher than the mean drug level in humans taking the highest recommended dose (as measured by total enzyme inhibitory activity). This same drug also produced vestibulocochlear Wallerian-like degeneration and retinal ganglion cell chromatolysis in dogs treated for 14 weeks at 180 mg/kg/day, a dose which resulted in a mean plasma drug level similar to that seen with the 60 mg/kg/day dose.
When administered to juvenile rats (postnatal days [PND] 4 through 80 at 5-45 mg/kg/day), no drug related changes were observed at 5 mg/kg/day. At 15 and 45 mg/kg/day, altered body-weight gain was observed during the dosing and 52-day recovery periods as well as slight thinning of the corpus callosum at the end of the recovery period. This finding was not evident in rats examined at the completion of the dosing period and was not associated with any inflammatory or degenerative changes in the brain. The biological relevance of the corpus callosum finding is uncertain due to the absence of any other microscopic changes in the brain or peripheral nervous tissue and because it occurred at the end of the recovery period. Neurobehavioral changes (enhanced acoustic startle responses and increased errors in water-maze learning) combined with evidence of generalized toxicity were noted at 45 mg/kg/day during the later part of the recovery period. Serum pravastatin levels at 15 mg/kg/day are approximately ≥1 times (AUC) the maximum pediatric dose of 40 mg. No thinning of the corpus callosum was observed in rats dosed with pravastatin (≥250 mg/kg/day) beginning PND 35 for 3 months suggesting increased sensitivity in younger rats. PND 35 in a rat is approximately equivalent to an 8- to 12-year-old human child. Juvenile male rats given 90 times (AUC) the 40 mg dose had decreased fertility (20%) with sperm abnormalities compared to controls.
14. Clinical Studies
14.1 Prevention of Coronary Heart Disease
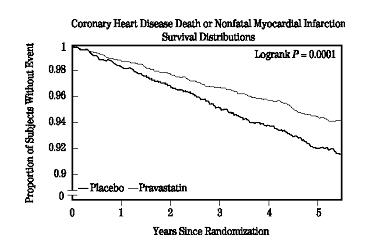
In the Pravastatin Primary Prevention Study (WOS),3 the effect of PRAVACHOL on fatal and nonfatal CHD was assessed in 6595 men 45 to 64 years of age, without a previous MI, and with LDL-C levels between 156 to 254 mg/dL (4-6.7 mmol/L). In this randomized, double-blind, placebo-controlled study, patients were treated with standard care, including dietary advice, and either PRAVACHOL 40 mg daily (N=3302) or placebo (N=3293) and followed for a median duration of 4.8 years. Median (25th, 75th percentile) percent changes from baseline after 6 months of pravastatin treatment in Total-C, LDL-C, TG, and HDL-C were −20.3 (−26.9, −11.7), −27.7 (−36.0, −16.9), −9.1 (−27.6, 12.5), and 6.7 (−2.1, 15.6), respectively.
PRAVACHOL significantly reduced the rate of first coronary events (either CHD death or nonfatal MI) by 31% (248 events in the placebo group [CHD death=44, nonfatal MI=204] versus 174 events in the PRAVACHOL group [CHD death=31, nonfatal MI=143], p=0.0001 [see figure below]). The risk reduction with PRAVACHOL was similar and significant throughout the entire range of baseline LDL cholesterol levels. This reduction was also similar and significant across the age range studied with a 40% risk reduction for patients younger than 55 years and a 27% risk reduction for patients 55 years and older. The Pravastatin Primary Prevention Study included only men, and therefore it is not clear to what extent these data can be extrapolated to a similar population of female patients.
PRAVACHOL also significantly decreased the risk for undergoing myocardial revascularization procedures (coronary artery bypass graft [CABG] surgery or percutaneous transluminal coronary angioplasty [PTCA]) by 37% (80 vs 51 patients, p=0.009) and coronary angiography by 31% (128 vs 90, p=0.007). Cardiovascular deaths were decreased by 32% (73 vs 50, p=0.03) and there was no increase in death from non-cardiovascular causes.
14.2 Secondary Prevention of Cardiovascular Events
In the LIPID4 study, the effect of PRAVACHOL, 40 mg daily, was assessed in 9014 patients (7498 men; 1516 women; 3514 elderly patients [age ≥65 years]; 782 diabetic patients) who had experienced either an MI (5754 patients) or had been hospitalized for unstable angina pectoris (3260 patients) in the preceding 3 to 36 months. Patients in this multicenter, double-blind, placebo-controlled study participated for an average of 5.6 years (median of 5.9 years) and at randomization had Total-C between 114 and 563 mg/dL (mean 219 mg/dL), LDL-C between 46 and 274 mg/dL (mean 150 mg/dL), TG between 35 and 2710 mg/dL (mean 160 mg/dL), and HDL-C between 1 and 103 mg/dL (mean 37 mg/dL). At baseline, 82% of patients were receiving aspirin and 76% were receiving antihypertensive medication. Treatment with PRAVACHOL significantly reduced the risk for total mortality by reducing coronary death (see Table 5). The risk reduction due to treatment with PRAVACHOL on CHD mortality was consistent regardless of age. PRAVACHOL significantly reduced the risk for total mortality (by reducing CHD death) and CHD events (CHD mortality or nonfatal MI) in patients who qualified with a history of either MI or hospitalization for unstable angina pectoris.
Table 5. LIPID - Primary and Secondary Endpoints:
| Number (%) of Subjects | ||||
|---|---|---|---|---|
| Event | Pravastatin 40 mg (N=4512) | Placebo (N=4502) | Risk Reduction | p-value |
| Primary Endpoint | ||||
| CHD mortality | 287 (6.4) | 373 (8.3) | 24% | 0.0004 |
| Secondary Endpoints | ||||
| Total mortality | 498 (11.0) | 633 (14.1) | 23% | <0.0001 |
| CHD mortality or nonfatal MI | 557 (12.3) | 715 (15.9) | 24% | <0.0001 |
| Myocardial revascularization procedures (CABG or PTCA) | 584 (12.9) | 706 (15.7) | 20% | <0.0001 |
| Stroke | ||||
| All-cause | 169 (3.7) | 204 (4.5) | 19% | 0.0477 |
| Non-hemorrhagic | 154 (3.4) | 196 (4.4) | 23% | 0.0154 |
| Cardiovascular mortality | 331 (7.3) | 433 (9.6) | 25% | <0.0001 |
In the CARE5 study, the effect of PRAVACHOL, 40 mg daily, on CHD death and nonfatal MI was assessed in 4159 patients (3583 men and 576 women) who had experienced a MI in the preceding 3 to 20 months and who had normal (below the 75th percentile of the general population) plasma total cholesterol levels. Patients in this double-blind, placebo-controlled study participated for an average of 4.9 years and had a mean baseline Total-C of 209 mg/dL. LDL-C levels in this patient population ranged from 101 to 180 mg/dL (mean 139 mg/dL). At baseline, 84% of patients were receiving aspirin and 82% were taking antihypertensive medications. Median (25th, 75th percentile) percent changes from baseline after 6 months of pravastatin treatment in Total-C, LDL-C, TG, and HDL-C were −22.0 (−28.4, −14.9), −32.4 (−39.9, −23.7), −11.0 (−26.5, 8.6), and 5.1 (−2.9, 12.7), respectively. Treatment with PRAVACHOL significantly reduced the rate of first recurrent coronary events (either CHD death or nonfatal MI), the risk of undergoing revascularization procedures (PTCA, CABG), and the risk for stroke or TIA (see Table 6).
Table 6. CARE - Primary and Secondary Endpoints:
| Number (%) of Subjects | ||||
|---|---|---|---|---|
| Event | Pravastatin 40 mg (N=2081) | Placebo (N=2078) | Risk Reduction | p-value |
| Primary Endpoint | ||||
| CHD mortality or nonfatal MIa | 212 (10.2) | 274 (13.2) | 24% | 0.003 |
| Secondary Endpoints | ||||
| Myocardial revascularization procedures (CABG or PTCA) | 294 (14.1) | 391 (18.8) | 27% | <0.001 |
| Stroke or TIA | 93 (4.5) | 124 (6.0) | 26% | 0.029 |
a The risk reduction due to treatment with PRAVACHOL was consistent in both sexes.
In the PLAC I6 study, the effect of pravastatin therapy on coronary atherosclerosis was assessed by coronary angiography in patients with coronary disease and moderate hypercholesterolemia (baseline LDL-C range: 130-190 mg/dL). In this double-blind, multicenter, controlled clinical trial, angiograms were evaluated at baseline and at 3 years in 264 patients. Although the difference between pravastatin and placebo for the primary endpoint (per-patient change in mean coronary artery diameter) and 1 of 2 secondary endpoints (change in percent lumen diameter stenosis) did not reach statistical significance, for the secondary endpoint of change in minimum lumen diameter, statistically significant slowing of disease was seen in the pravastatin treatment group (p=0.02).
In the REGRESS7 study, the effect of pravastatin on coronary atherosclerosis was assessed by coronary angiography in 885 patients with angina pectoris, angiographically documented coronary artery disease, and hypercholesterolemia (baseline total cholesterol range: 160-310 mg/dL). In this double-blind, multicenter, controlled clinical trial, angiograms were evaluated at baseline and at 2 years in 653 patients (323 treated with pravastatin). Progression of coronary atherosclerosis was significantly slowed in the pravastatin group as assessed by changes in mean segment diameter (p=0.037) and minimum obstruction diameter (p=0.001).
Analysis of pooled events from PLAC I, PLAC II,8 REGRESS, and KAPS9 studies (combined N=1891) showed that treatment with pravastatin was associated with a statistically significant reduction in the composite event rate of fatal and nonfatal MI (46 events or 6.4% for placebo versus 21 events or 2.4% for pravastatin, p=0.001). The predominant effect of pravastatin was to reduce the rate of nonfatal MI.
14.3 Primary Hypercholesterolemia (Fredrickson Types IIa and IIb)
PRAVACHOL is highly effective in reducing Total-C, LDL-C, and TG in patients with heterozygous familial, presumed familial combined, and non-familial (non-FH) forms of primary hypercholesterolemia, and mixed dyslipidemia. A therapeutic response is seen within 1 week, and the maximum response usually is achieved within 4 weeks. This response is maintained during extended periods of therapy. In addition, PRAVACHOL is effective in reducing the risk of acute coronary events in hypercholesterolemic patients with and without previous MI.
A single daily dose is as effective as the same total daily dose given twice a day. In multicenter, double-blind, placebo-controlled studies of patients with primary hypercholesterolemia, treatment with pravastatin in daily doses ranging from 10 to 40 mg consistently and significantly decreased Total-C, LDL-C, TG, and Total-C/HDL-C and LDL-C/HDL-C ratios (see Table 7).
In a pooled analysis of 2 multicenter, double-blind, placebo-controlled studies of patients with primary hypercholesterolemia, treatment with pravastatin at a daily dose of 80 mg (N=277) significantly decreased Total-C, LDL-C, and TG. The 25th and 75th percentile changes from baseline in LDL-C for pravastatin 80 mg were −43% and −30%. The efficacy results of the individual studies were consistent with the pooled data (see Table 7).
Treatment with PRAVACHOL modestly decreased VLDL-C and PRAVACHOL across all doses produced variable increases in HDL-C (see Table 7).
Table 7. Primary Hypercholesterolemia Studies: Dose Response of PRAVACHOL Once Daily Administration:
| Dose | Total-C | LDL-C | HDL-C | TG |
|---|---|---|---|---|
| Mean Percent Changes From Baseline After 8 Weeksa | ||||
| Placebo (N=36) | −3% | −4% | +1% | −4% |
| 10 mg (N=18) | −16% | −22% | +7% | −15% |
| 20 mg (N=19) | −24% | −32% | +2% | −11% |
| 40 mg (N=18) | −25% | −34% | +12% | −24% |
| Mean Percent Changes From Baseline After 6 Weeksb | ||||
| Placebo (N=162) | 0% | −1% | −1% | +1% |
| 80 mg (N=277) | −27% | −37% | +3% | −19% |
a A multicenter, double-blind, placebo-controlled study.
b Pooled analysis of 2 multicenter, double-blind, placebo-controlled studies.
In another clinical trial, patients treated with pravastatin in combination with cholestyramine (70% of patients were taking cholestyramine 20 or 24 g per day) had reductions equal to or greater than 50% in LDL-C. Furthermore, pravastatin attenuated cholestyramine-induced increases in TG levels (which are themselves of uncertain clinical significance).
14.4 Hypertriglyceridemia (Fredrickson Type IV)
The response to pravastatin in patients with Type IV hyperlipidemia (baseline TG >200 mg/dL and LDL-C <160 mg/dL) was evaluated in a subset of 429 patients from the CARE study. For pravastatin-treated subjects, the median (min, max) baseline TG level was 246.0 (200.5, 349.5) mg/dL (see Table 8).
Table 8. Patients with Fredrickson Type IV Hyperlipidemia Median (25th, 75th percentile) % Change from Baseline:
| Pravastatin 40 mg (N=429) | Placebo (N=430) | |
|---|---|---|
| TG | −21.1 (−34.8, 1.3) | −6.3 (−23.1, 18.3) |
| Total-C | −22.1 (−27.1, −14.8) | 0.2 (−6.9, 6.8) |
| LDL-C | −31.7 (−39.6, −21.5) | 0.7 (−9.0, 10.0) |
| HDL-C | 7.4 (−1.2, 17.7) | 2.8 (−5.7, 11.7) |
| Non-HDL-C | −27.2 (−34.0, −18.5) | −0.8 (−8.2, 7.0) |
14.5 Dysbetalipoproteinemia (Fredrickson Type III)
The response to pravastatin in two double-blind crossover studies of 46 patients with genotype E2/E2 and Fredrickson Type III dysbetalipoproteinemia is shown in Table 9.
Table 9. Patients with Fredrickson Type III Dysbetalipoproteinemia Median (min, max) % Change from Baseline:
| Median (min, max) at Baseline (mg/dL) | Median % Change (min, max) Pravastatin 40 mg (N=20) | |
|---|---|---|
| Study 1 | ||
| Total-C | 386.5 (245.0, 672.0) | −32.7 (−58.5, 4.6) |
| TG | 443.0 (275.0, 1299.0) | −23.7 (−68.5, 44.7) |
| VLDL-Ca | 206.5 (110.0, 379.0) | −43.8 (−73.1, −14.3) |
| LDL-Ca | 117.5 (80.0, 170.0) | −40.8 (−63.7, 4.6) |
| HDL-C | 30.0 (18.0, 88.0) | 6.4 (−45.0, 105.6) |
| Non-HDL-C | 344.5 (215.0, 646.0) | −36.7 (−66.3, 5.8) |
| a N=14 | ||
| Median (min, max) at Baseline (mg/dL) | Median % Change (min, max) Pravastatin 40 mg (N=26) | |
| Study 2 | ||
| Total-C | 340.3 (230.1, 448.6) | −31.4 (−54.5, −13.0) |
| TG | 343.2 (212.6, 845.9) | −11.9 (−56.5, 44.8) |
| VLDL-C | 145.0 (71.5, 309.4) | −35.7 (−74.7, 19.1) |
| LDL-C | 128.6 (63.8, 177.9) | −30.3 (−52.2, 13.5) |
| HDL-C | 38.7 (27.1, 58.0) | 5.0 (−17.7, 66.7) |
| Non-HDL-C | 295.8 (195.3, 421.5) | −35.5 (−81.0, −13.5) |
14.6 Pediatric Clinical Study
A double-blind, placebo-controlled study in 214 patients (100 boys and 114 girls) with heterozygous familial hypercholesterolemia (HeFH), aged 8 to 18 years was conducted for 2 years. The children (aged 8-13 years) were randomized to placebo (N=63) or 20 mg of pravastatin daily (N=65) and the adolescents (aged 14-18 years) were randomized to placebo (N=45) or 40 mg of pravastatin daily (N=41). Inclusion in the study required an LDL-C level >95th percentile for age and sex and one parent with either a clinical or molecular diagnosis of familial hypercholesterolemia. The mean baseline LDL-C value was 239 mg/dL and 237 mg/dL in the pravastatin (range: 151-405 mg/dL) and placebo (range: 154-375 mg/dL) groups, respectively.
Pravastatin significantly decreased plasma levels of LDL-C, Total-C, and ApoB in both children and adolescents (see Table 10). The effect of pravastatin treatment in the 2 age groups was similar.
Table 10. Lipid-Lowering Effects of Pravastatin in Pediatric Patients with Heterozygous Familial Hypercholesterolemia: Least-Squares Mean % Change from Baseline at Month 24 (Last Observation Carried Forward: Intent-to-Treat)a:
| Pravastatin 20 mg (Aged 8-13 years) N=65 | Pravastatin 40 mg (Aged 14-18 years) N=41 | Combined Pravastatin (Aged 8-18 years) N=106 | Combined Placebo (Aged 8-18 years) N=108 | 95% CI of the Difference Between Combined Pravastatin and Placebo | |
|---|---|---|---|---|---|
| LDL-C | −26.04b | −21.07b | −24.07b | −1.52 | (−26.74, −18.86) |
| TC | −20.75b | −13.08b | −17.72b | −0.65 | (−20.40, −13.83) |
| HDL-C | 1.04 | 13.71 | 5.97 | 3.13 | (−1.71, 7.43) |
| TG | −9.58 | −0.30 | −5.88 | −3.27 | (−13.95, 10.01) |
| ApoB (N) | −23.16b (61) | −18.08b (39) | −21.11b (100) | −0.97 (106) | (−24.29, −16.18) |
a The above least-squares mean values were calculated based on log-transformed lipid values.
b Significant at p≤0.0001 when compared with placebo.
The mean achieved LDL-C was 186 mg/dL (range: 67-363 mg/dL) in the pravastatin group compared to 236 mg/dL (range: 105-438 mg/dL) in the placebo group.
The safety and efficacy of pravastatin doses above 40 mg daily have not been studied in children. The long-term efficacy of pravastatin therapy in childhood to reduce morbidity and mortality in adulthood has not been established.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.