QAIALDO Oral suspension Ref.[51071] Active ingredients: Spironolactone
Source: European Medicines Agency (EU) Revision Year: 2026 Publisher: Lipomed GmbH, Hegenheimer Strasse 2, 79576 Weil am Rhein, Germany
4.1. Therapeutic indications
In the management of refractory oedema associated with congestive cardiac failure; hepatic cirrhosis with ascites and oedema, malignant ascites, nephrotic syndrome, diagnosis and treatment of primary aldosteronism, essential hypertension.
Neonates, children and adolescents should only be treated under guidance of a paediatric specialist. There is limited paediatric data available (see sections 5.1 and 5.2).
4.2. Posology and method of administration
Posology
Adults
Congestive heart failure with oedema
Usual dose - 100 mg/day. In difficult or severe cases the dose may be gradually increased up to 200 mg/day. When oedema is controlled, the usual maintenance level is 75 mg/day to 200 mg/day.
Severe heart failure in conjunction with standard therapy (New York Heart Association Class III-IV)
Based on the randomized aldactone evaluation study (RALES), treatment in conjunction with standard therapy should be initiated at a dose of spironolactone 25 mg once daily in patients with a serum potassium ≤5.0 mEq/L and serum creatinine ≤2.5 mg/dL. Patients who tolerate 25 mg once daily may have their dose increased to 50 mg once daily as clinically indicated. Patients who do not tolerate 25 mg once daily may have their dose reduced to 25 mg every other day. See section 4.4 for advice on monitoring serum potassium and serum creatinine.
Hepatic cirrhosis with ascites and oedema
If urinary Na+/K+ ratio is greater than 1.0, 100 mg per day. If the ratio is less than 1.0, 200 mg/day to 400 mg/day. Maintenance dose should be individually determined.
Malignant ascites
Initial dose usually 100 mg/day to 200 mg/day. In severe cases the dose may be gradually increased up to 400 mg/day. When oedema is controlled, maintenance dose should be individually determined.
Nephrotic syndrome
Usual dose – 100 mg/day to 200 mg/day. Spironolactone has not been shown to be anti-inflammatory, nor to affect the basic pathological process. Its use is only advised if glucocorticoids by themselves are insufficiently effective.
Diagnosis and treatment of primary aldosteronism
Spironolactone may be employed as an initial diagnostic measure to provide presumptive evidence of primary hyperaldosteronism while patients are on normal diets.
- Long test: Spironolactone is administered at a daily dose of 400 mg for 3 to 4 weeks. Correction of hypokalaemia and of hypertension provides presumptive evidence for the diagnosis of primary hyperaldosteronism.
- Short test: Spironolactone is administered at a daily dose of 400 mg for 4 days. If serum potassium increases during spironolactone administration but drops when spironolactone is discontinued, a presumptive diagnosis of primary hyperaldosteronism should be considered.
After the diagnosis of hyperaldosteronism has been established by more definitive testing procedures, spironolactone may be administered in doses of 100 mg to 400 mg daily in preparation for surgery. For patients who are considered unsuitable for surgery, Spironolactone may be employed for long term maintenance therapy at the lowest effective dose determined for the individual patient.
Essential hypertension
Usual dose – 50 mg/day to 100 mg/day, which for difficult or severe cases may be gradually increased at 2 weekly intervals up to 200 mg/day. Treatment should be continued for 2 weeks or longer since an adequate response may not occur before this time. Dose should subsequently be adjusted according to the response of the patient.
Special populations
Elderly
It is recommended that treatment is started with the lowest dose and titrated upwards as required to achieve maximum benefit. Care should be taken in severe hepatic and renal impairment which may alter spironolactone metabolism and excretion.
Renal/hepatic impairment
Patients with mild renal impairment (glomerular filtration rate (GFR) 60 – 90 ml/min) should be started on the lowest dose. Serum potassium levels and renal function should be monitored closely. Spironolactone is contraindicated in patients with moderate (GFR 30 - <60 ml/min) to severe (GFR <30 ml/min) renal impairment (see sections 4.3 and 4.4).
Since impaired hepatic function may result in reduced elimination of spironolactone and its metabolites, patients with impaired hepatic function should be started on the lowest dose and titrated slowly. Patients should be monitored for dose related adverse reactions (see section 4.4).
Paediatric population
Initiate treatment with the smallest dose and adjust on the basis of response and tolerance (see sections 4.3 and 4.4).
Diuresis in congestive heart failure, ascites, oedema and nephrotic syndrome:
- Neonate: 1-2 mg/kg/daily in 1-2 divided doses.
- Infant or child 1 month to 18 years: 1-3 mg/kg daily in 1-2 divided doses (maximum 200 mg daily).
Primary hyperaldosteronism; resistant ascites:
- Neonate: up to a maximum of 7 mg/kg daily may be used.
- Infant or Child 1 month to 18 years: up to a maximum of 9 mg/kg daily (total maximum 400 mg daily) may be used.
Neonates, children and adolescents should only be treated under guidance of a paediatric specialist. There is limited paediatric data available (see sections 5.1 and 5.2).
The paediatric table below shows, for a range of ages, weight and doses, the dose (mg) to volume (ml) conversion using the two oral syringes.
Table 1. Dose (mg) to volume (ml) conversion using oral syringe. Daily doses are displaye:
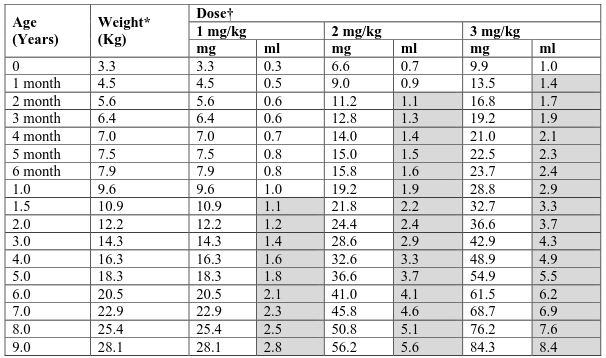
* 50th percentile for boys extracted from WHO (0-10 years) growth charts
† Doses less than or equal to 10 mg to be drawn up using the 1 ml oral syringe. Doses greater than 10 mg to be drawn up using the 5 ml oral syringe or a combination of both syringes (shaded cells).
Method of administration
Spironolactone should be taken together with a meal.
This medicinal product is for oral use. The bottle should be shaken thoroughly before use for redispersing the suspension.
Two dosing syringes (a 1 ml syringe and a 5 ml syringe) are provided for accurate measurement of the prescribed dose of the oral suspension.
The smaller 1 ml syringe is for measuring doses of less than or equal to 10 mg. The syringe is marked at 0.1 ml intervals, allowing for dosing in 1 mg increments.
The larger 5 ml syringe is for measuring doses more than 10 mg. The syringe has graduations at every 0.2 ml (2 mg) and is marked at 1 ml intervals and at 2.5 ml. Each 1 ml contains 10 mg of spironolactone.
The healthcare professional should advise the patient or carer which syringe to use to ensure that the correct volume is administered.
The healthcare professional should advise the patient or carer to place the tip of the syringe into the mouth and to the inside of the cheek, and the contents gently released. To assist accurate and consistent dose delivery to the stomach, water should be taken after each dose of spironolactone. In adults without swallowing difficulties, solid oral formulations may be more appropriate and convenient.
4.9. Overdose
Symptoms
Acute overdose may be manifested by drowsiness, mental confusion, nausea, vomiting, dizziness, diarrhoea or maculopapular or erythematous rash. Dehydration may occur. Hyponatraemia or hyperkalaemia may be induced but these effects are unlikely to be associated with acute overdose. See section 4.8 for the symptoms of hyperkalaemia.
Treatment
No specific antidote has been identified. Spironolactone use should be discontinued. Improvement may be expected after withdrawal of the medicinal product. General supportive measures including replacement of fluids and electrolytes may be indicated. For hyperkalaemia, reduce potassium intake, administer potassium-excreting diuretics, intravenous glucose with regular insulin, or oral ionexchange resins.
6.3. Shelf life
Unopened bottle: 2 years.
After first opening: Keep the bottle tightly closed and store below 25°C. Discard any unused contents after 12 weeks.
6.4. Special precautions for storage
Before first opening, this medicinal product does not require any special storage conditions.
For storage conditions after first opening, see section 6.3.
6.5. Nature and contents of container
Amber type III glass bottle with tamper evident child-resistant closure (high density polyethylene-HDPE with expanded polyethylene liner) containing 150 ml of oral suspension.
Each pack contains one bottle, a low density polyethylene (LDPE) bottle adaptor and 2 dosing syringes (a 1 ml syringe graduated in 0.01 ml increments and a 5 ml syringe graduated in 0.2 ml increments).
6.6. Special precautions for disposal and other handling
The bottle should be shaken thoroughly before use to ensure the oral suspension is well mixed.
Any unused product or waste material should be disposed of in accordance with local requirements.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.