RADICAVA Solution for injection Ref.[10273] Active ingredients: Edaravone
Source: FDA, National Drug Code (US) Revision Year: 2018
12.1. Mechanism of Action
The mechanism by which RADICAVA exerts its therapeutic effect in patients with ALS is unknown.
12.3. Pharmacokinetics
RADICAVA is administered by IV infusion. The maximum plasma concentration (Cmax) of edaravone was reached by the end of infusion. There was a trend of more than dose-proportional increase in area under the concentration-time curve (AUC) and Cmax of edaravone. With multiple-dose administration, edaravone does not accumulate in plasma.
Distribution
Edaravone is bound to human serum proteins (92%), mainly to albumin, with no concentration dependence in the range of 0.1 to 50 micromol/L.
Elimination
The mean terminal elimination half-life of edaravone is 4.5 to 6 hours. The half-lives of its metabolites are 2 to 2.8 hours.
Metabolism
Edaravone is metabolized to a sulfate conjugate and a glucuronide conjugate, which are not pharmacologically active. The glucuronide conjugation of edaravone involves multiple uridine diphosphate glucuronosyltransferase (UGT) isoforms (UGT1A6, UGT1A9, UGT2B7, and UGT2B17) in the liver and kidney. In human plasma, edaravone is mainly detected as the sulfate conjugate, which is presumed to be formed by sulfotransferases.
Excretion
In Japanese and Caucasian healthy volunteer studies, edaravone was excreted mainly in the urine as its glucuronide conjugate form (70-90% of the dose). Approximately 5-10% of the dose was recovered in the urine as sulfate conjugate, and only 1% of the dose or less was recovered in the urine as unchanged form. In vitro studies suggest that sulfate conjugate of edaravone is hydrolyzed back to edaravone, which is then converted to the glucuronide conjugate in the human kidney before excretion into the urine.
Specific Populations
Geriatric Patients
No age effect on edaravone pharmacokinetics has been found [see Use in Specific Populations (8.5)].
Patients with Renal and Hepatic Impairment
No pharmacokinetic data are available in patients with renal impairment or hepatic impairment [see Use in Specific Populations (8.6,8.7)].
Male and Female Patients
No gender effect on edaravone pharmacokinetics has been found.
Racial or Ethnic Groups
There were no significant racial differences in Cmax and AUC of edaravone between Japanese and Caucasian subjects.
Drug Interaction Studies
The pharmacokinetics of edaravone is not expected to be significantly affected by inhibitors of CYP enzymes, UGTs, or major transporters.
In vitro studies demonstrated that, at clinical dose, edaravone and its metabolites are not expected to significantly inhibit cytochrome P450 enzymes (CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, CYP3A4), UGT1A1, UGT2B7, or transporters (P-gp, BCRP, OATP1B1, OATP1B3, OAT1, OAT3, and OCT2) in humans. Edaravone and its metabolites are not expected to induce CYP1A2, CYP2B6, or CYP3A4 at the clinical dose level of RADICAVA.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
The carcinogenic potential of edaravone has not been adequately assessed.
Mutagenesis
Edaravone was negative in in vitro (bacterial reverse mutation and Chinese hamster lung chromosomal aberration) and in vivo (mouse micronucleus) assays.
Impairment of Fertility
Intravenous administration of edaravone (0, 3, 20, or 200 mg/kg) prior to and throughout mating in males and females and continuing in females to gestation day 7 had no effect on fertility; however, disruption of the estrus cycle and mating behavior was observed at the highest dose tested. No effects on reproductive function were observed at the lower doses, which are up to 3 times the RHD of 60 mg, on a body surface area (mg/m²) basis.
14. Clinical Studies
The efficacy of RADICAVA for the treatment of ALS was established in a 6-month, randomized, placebo-controlled, double-blind study conducted in Japanese patients with ALS who were living independently and met the following criteria at screening:
- Functionality retained most activities of daily living (defined as scores of 2 points or better on each individual item of the ALS Functional Rating Scale – Revised [ALSFRS-R; described below])
- Normal respiratory function (defined as percent-predicted forced vital capacity values of [%FVC] ≥80%)
- Definite or Probable ALS based on El Escorial revised criteria
- Disease duration of 2 years or less
The study enrolled 69 patients in the RADICAVA arm and 68 in the placebo arm. Baseline characteristics were similar between these groups, with over 90% of patients in each group being treated with riluzole.
RADICAVA was administered as an intravenous infusion of 60 mg given over a 60 minute period according to the following schedule:
- An initial treatment cycle with daily dosing for 14 days, followed by a 14-day drug-free period (Cycle 1)
- Subsequent treatment cycles with daily dosing for 10 days out of 14-day periods, followed by 14-day drug-free periods (Cycles 2-6).
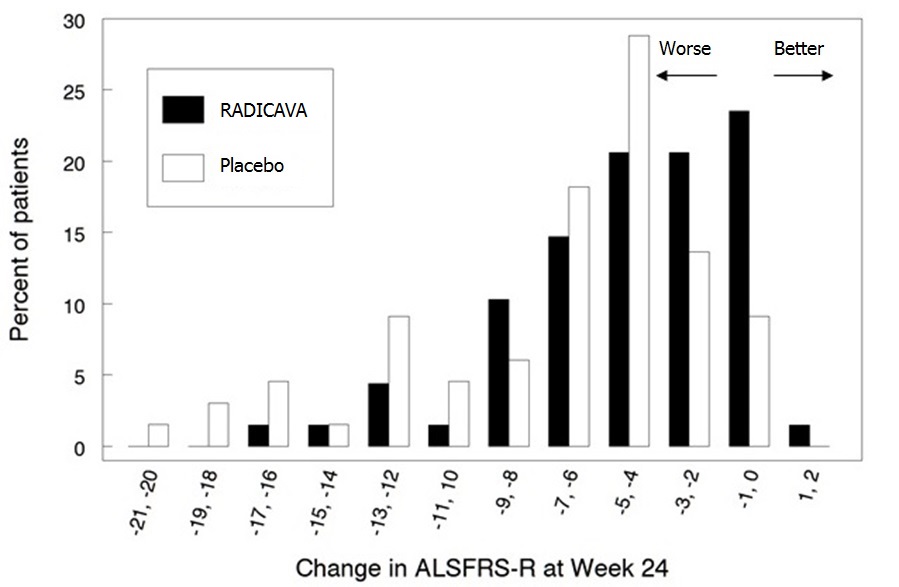
The primary efficacy endpoint was a comparison of the change between treatment arms in the ALSFRS-R total scores from baseline to Week 24. The ALSFRS-R scale consists of 12 questions that evaluate the fine motor, gross motor, bulbar, and respiratory function of patients with ALS (speech, salivation, swallowing, handwriting, cutting food, dressing/hygiene, turning in bed, walking, climbing stairs, dyspnea, orthopnea, and respiratory insufficiency). Each item is scored from 0-4, with higher scores representing greater functional ability. The decline in ALSFRS-R scores from baseline was significantly less in the RADICAVA-treated patients as compared to placebo (see Table 2). The distribution of change in ALSFRS-R scores from baseline to Week 24 by percent of patients is shown in Figure 1.
Table 2. Analysis of Change from Baseline to Week 24 in ALSFRS-R Scores:
| Treatment | Change from Baseline LS Mean ± SE (95% CI) | Treatment Difference (RADICAVA – placebo [95% CI]) | p-value |
|---|---|---|---|
| RADICAVA 60mg | −5.01±0.64 | 2.49 (0.99, 3.98) | 0.0013 |
| Placebo | −7.50±0.66 |
Figure 1. Distribution of Change from Baseline to Week 24 in ALSFRS-R Scores:
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.