REMOVAB Concentrate for solution for infusion Ref.[27988] Active ingredients: Catumaxomab
Source: European Medicines Agency (EU) Revision Year: 2017 Publisher: Neovii Biotech GmbH, Am Haag 6-7, 82166 Graefelfing, Germany
5.1. Pharmacodynamic properties
Pharmacotherapeutic group: Antineoplastic agents, monoclonal antibodies
ATC code: L01XC09
Mechanism of action
Catumaxomab is a trifunctional rat-mouse hybrid monoclonal antibody that is specifically directed against the epithelial cell adhesion molecule (EpCAM) and the CD3 antigen. The EpCAM antigen is overexpressed on most carcinomas (Table 2). CD3 is expressed on mature T-cells as a component of the T-cell receptor. A third functional binding site in the Fc-region of catumaxomab enables interaction with accessory immune cells via Fcγ receptors. Due to catumaxomab’s binding properties, tumour cells, T-cells and accessory immune cells come in close proximity. Thereby, a concerted immunoreaction against tumour cells is induced which includes different mechanisms of action such as T-cell activation, antibody-dependent cell-mediated cytotoxicity (ADCC), complement-dependent cytotoxicity (CDC) and phagocytosis. This results in destruction of tumour cells.
Table 2. EpCAM expression in most relevant ascites causing cancer types:
| Δεδομένα βιβλιογραφίας | Retrospective data from study IP-CAT-AC-03 | ||
|---|---|---|---|
| Cancer Type | Percentage of tumors expressing EpCAM | Percentage of EpCAM positive effusion | Percentage of EpCAM positive effusions |
| Ovarian | 90-92 | 79-100 | 98 |
| Gastric | 96 | 75-100 | 100 |
| Colon | 100 | 87-100 | 100 |
| Pancreatic | 98 | 83-100 | 80 |
| Breast | 45*-81 | 71-100 | 86 |
| Endometrial | 94 | 100 | 100 |
* = lobular breast cancer
Pharmacodynamic effects
The anti-tumour activity of catumaxomab has been demonstrated in vitro and in vivo. Effective catumaxomab-mediated killing of tumour cells in vitro was observed for target cells with low and high expression of the EpCAM antigen, independent of the primary tumour type. The in vivo anti-tumour activity of catumaxomab was confirmed in an immunologically compromised mouse model of ovarian carcinoma, where tumour development was delayed by an intraperitoneal treatment with catumaxomab and human peripheral blood mononuclear cells.
Clinical efficacy
The efficacy of catumaxomab was demonstrated in two phase III clinical studies. Patients of nonCaucasian origin have not been included in these clinical studies.
IP-REM-AC-01
A pivotal, two-arm, randomised, open-label, phase II/III clinical trial in 258 patients with symptomatic malignant ascites due to EpCAM-positive carcinomas of whom 170 were randomised to catumaxomab treatment. This study compared paracentesis plus catumaxomab versus paracentesis alone (control).
Catumaxomab was applied in patients where standard therapy was not available or no longer feasible and who had a Karnofsky performance status of at least 60. Catumaxomab was administered as four intraperitoneal infusions with increased doses of 10, 20, 50 and 150 micrograms on day 0, 3, 7 and 10, respectively (see section 4.2). In the pivotal study IP-REM-AC-01 98.1% of patients were hospitalised for a median of 11 days.
In this study, the primary efficacy endpoint was puncture-free survival, which was a composite endpoint defined as the time to first need for therapeutic ascites puncture or death, whichever occurred first. The results for puncture-free survival and time to first need for therapeutic ascites puncture in terms of medians and hazard ratios are presented in Table 3. Kaplan Meier estimates for time to first need for therapeutic ascites puncture are given in Figure 1.
Table 3. Efficacy results (puncture-free survival and time to first need for therapeutic ascites puncture) of study IP-REM-AC-01:
| Variable | Paracentesis + catumaxomab (N=170) | Paracentesis (control) (N=88) |
|---|---|---|
| Puncture free survival | ||
| Median puncture-free survival (days) | 44 | 11 |
| 95% CI for median (days) | [31; 49] | [9; 16] |
| p-value (log-rank test) | <0.0001 | |
| Hazard ratio (HR) | 0.310 | |
| 95% CI for HR | [0.228; 0.423] | |
| Time to first need for therapeutic ascites puncture | ||
| Median time to first need for therapeutic ascites puncture (days) | 77 | 13 |
| 95% CI for median (days) | [62; 104] | [9; 17] |
| p-value (log-rank test) | <0.0001 | |
| Hazard ratio (HR) | 0.169 | |
| 95% CI for HR | [0.114; 0.251] | |
Figure 1. Kaplan-Meier estimates of time to first need for therapeutic ascites puncture of study IP-REM-AC-01:
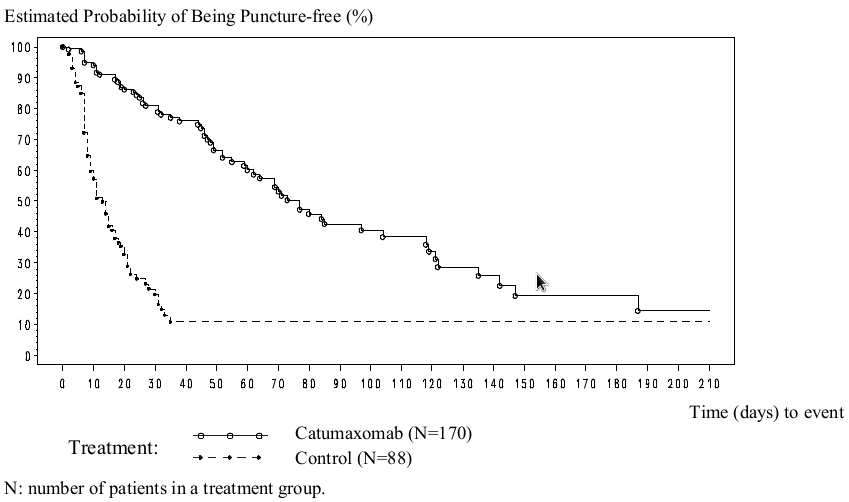
The efficacy of the treatment with paracentesis and catumaxomab in patients with malignant ascites due to EpCAM-positive carcinomas was statistically significantly superior to that with paracentesis alone in terms of puncture-free survival and time to first need for therapeutic ascites puncture.
After completion of the study, patients were further observed until the end of their lifetime to assess overall survival (Table 4).
Table 4. Overall survival of study IP-REM-AC-01 in post study phase:
| Paracentesis + catumaxomab (N=170) | Paracentesis (control) (N=88) | |
|---|---|---|
| Hazard ratio (HR) | 0.798 | |
| 95% CI for HR | [0.606; 1.051] | |
| 6 months survival rate | 27.5% | 17.1% |
| 1 year survival rate | 11.4% | 2.6% |
| Median overall survival (days) | 72 | 71 |
| 95% CI for median (days) | [61; 98] | [54; 89] |
| p-value (log-rank test | 0.1064 | |
Altogether 45 out of 88 (51%) patients in the control arm crossed-over to achieve active treatment with catumaxomab.
IP-CAT-AC-03
This confirmatory two-arm, randomized, open label, phase IIIb study in 219 epithelial cancer patients with symptomatic malignant ascites requiring therapeutic ascites puncture investigated treatment with catumaxomab plus 25 mg prednisolone premedication vs. catumaxomab alone. Catumaxomab was administered as four 3-hour constant-rate i.p. infusions in doses of 10, 20, 50 and 150 micrograms on day 0, 3, 7 and 10, respectively, in both groups. The patient population was comparable to the pivotal study.
In order to assess the impact of prednisolone premedication on safety and efficacy the primary safety endpoint “composite safety score” and the co-primary efficacy endpoint “puncture-free survival” were investigated.
The composite safety score evaluated the frequency and severity of the main known adverse reactions pyrexia, nausea, vomiting and abdominal pain in both treatment groups. Administration of prednisolone as premedication did not result in a reduction of these adverse reactions.
The primary efficacy endpoint, puncture-free survival, was a composite endpoint defined as the time to first need for therapeutic ascites puncture or death, whichever occurred first (identical to the pivotal study).
Table 5. Efficacy results (puncture-free survival and time to first need for therapeutic ascites puncture) of study IP-CAT-AC-03:
| Variable | Catumaxomab + prednisolone (N=111) | Catumaxomab (N=108) | Pooled population (N=219) |
|---|---|---|---|
| Puncture free survival | |||
| Median puncture-free survival (days) | 30 | 37 | 35 |
| 95% CI for median (days) | [23; 67] | [24; 61] | [26; 59] |
| p-value (log-rank test) | 0,402 | ||
| Hazard ratio (HR) (Catumaxomab versus Catumaxomab + Prednisolone) | 1.130 | ||
| 95% CI for HR | [0.845; 1.511] | ||
| Time to first need for therapeutic ascites puncture | |||
| Median time to first need for therapeutic ascites puncture (days) | 78 | 102 | 97 |
| 95% CI for median (days) | [30; 223] | [69; 159] | [67; 155] |
| p-value (log-rank test) | 0.599 | ||
| Hazard ratio (HR) (Catumaxomab versus Catumaxomab + Prednisolone) | 0.901 | ||
| 95% CI for HR | [0.608; 1.335] | ||
As secondary efficacy endpoint overall survival (Table 6) was assessed.
Table 6. Overall survival of study IP-CAT-AC-03 in post study phase:
| Catumaxomab + prednisolone (N=111) | Catumaxomab (N=108) | Pooled population (N=219) | |
|---|---|---|---|
| Median overall survival (days) | 124 | 86 | 103 |
| 95% CI for median (days) | [97.0; 169.0] | [72.0; 126.0] | [82; 133] |
| p-value (log-rank test) | 0.186 | ||
| Hazard ratio (HR) (Catumaxomab versus Catumaxomab + Prednisolone) | 1.221 | ||
| 95% CI for HR | [0.907; 1.645] | ||
Immunogenicity
The induction of human anti-murine (rat and/or mouse) antibodies (HAMAs/HARAs) is an intrinsic effect of murine monoclonal antibodies. Current data on catumaxomab derived from the pivotal study show that only 5.6% of patients (7/124 patients) were HAMA positive before the 4th infusion. HAMAs were present in 94% of patients one month after the last catumaxomab infusion. No hypersensitivity reactions were observed. Patients who developed HAMAs 8 days after catumaxomab treatment showed better clinical outcome, as measured by puncture-free survival, time to next puncture and overall survival, compared with HAMA-negative patients.
In a feasibility study evaluating a second i.p. infusion cycle consisting of 10, 20, 50 and 150 micrograms of catumaxomab in 8 patients with malignant ascites due to carcinoma (IP-CAT-AC-04) ADA was detectable in all available ascites and plasma samples at screening. The patients remained ADA positive during treatment phase and follow-up. Despite pre-existing ADA values all patients received all 4 catumaxomab infusions. The median puncture-free survival time was 47.5 days, median time to first therapeutic puncture 60.0 days and median overall survival 406.5 days. All patients experienced symptoms related to catumaxomab mode of action with a safety profile comparable in nature to the first i.p. treatment cycle. No hypersensitivity reactions were observed.
5.2. Pharmacokinetic properties
Pharmacokinetics of catumaxomab during and after four intraperitoneal infusions of 10, 20, 50 and 150 micrograms catumaxomab were investigated in 13 patients with symptomatic malignant ascites due to EpCAM-positive carcinomas.
The variability between subjects was high. The geometric mean plasma Cmax was approximately 0.5 ng/ml (range 0 to 2.3), and the geometric mean plasma AUC was approximately 1.7 day* ng/ml (range < LLOQ (lower limit of quantification) to 13.5). The geometric mean apparent terminal plasma elimination half-life (t1/2) was approximately 2.5 days (range 0.7 to 17).
Catumaxomab was detectable in the ascites fluid and in plasma. The concentrations increased with the number of infusions and the doses applied in most patients. Plasma levels tended to decline after achieving a maximum after each dose.
Special populations
No studies have been conducted.
5.3. Preclinical safety data
Administration of catumaxomab in animal models did not result in any signs of abnormal or drug-related acute toxicity or signs of local intolerance at the injection/infusion site. However, these findings are of limited value due to the high species-specificity of catumaxomab.
Repeated-dose toxicity, genotoxicity, carcinogenicity, reproductive and developmental toxicity studies have not been performed.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.