Source: FDA, National Drug Code (US) Revision Year: 2021
The mechanism of action of THALOMID is not fully understood. Cellular activities of thalidomide are mediated through its target cereblon, a component of a cullin ring E3 ubiquitin ligase enzyme complex. THALOMID possesses immunomodulatory, anti-inflammatory and antiangiogenic properties. Available data from in vitro studies and clinical trials suggest that the immunologic effects of this compound can vary substantially under different conditions, but may be related to suppression of excessive tumor necrosis factor-alpha (TNF-α) production and down-modulation of selected cell surface adhesion molecules involved in leukocyte migration. For example, administration of thalidomide has been reported to decrease circulating levels of TNF-α in patients with erythema nodosum leprosum (ENL); however, it has also been shown to increase plasma TNF-α levels in HIV-seropositive patients. Other anti-inflammatory and immunomodulatory properties of thalidomide may include suppression of macrophage involvement in prostaglandin synthesis, and modulation of interleukin-10 and interleukin-12 production by peripheral blood mononuclear cells. Thalidomide treatment of multiple myeloma patients is accompanied by an increase in the number of circulating natural killer cells, and an increase in plasma levels of interleukin-2 and interferon-gamma (T cell-derived cytokines associated with cytotoxic activity). Thalidomide was found to inhibit angiogenesis in a human umbilical artery explant model in vitro. The cellular processes of angiogenesis inhibited by thalidomide may include the proliferation of endothelial cells.
Absorption of THALOMID is slow after oral administration. The maximum plasma concentrations are reached approximately 2-5 hours after administration. The absolute bioavailability of thalidomide from thalidomide capsules has not yet been characterized in human subjects due to its poor aqueous solubility. Based on the 14C-radiolabel thalidomide study in human, greater than 90% of the total radioactivity is recovered in urine suggesting good oral absorption. While the extent of absorption (as measured by area under the curve [AUC]) is proportional to dose in healthy subjects, the observed peak concentration (Cmax) increased in a less than proportional manner (see Table 5 below). This lack of Cmax dose proportionality, coupled with the observed increase in Tmax values, suggests that the poor solubility of thalidomide in aqueous media may be hindering the rate of absorption.
Table 5. Pharmacokinetic Parameter Values for THALOMID Mean (%CV):
| Population/ Single Dose | AUC0-∞ mcg∙hr/mL | Cmax mcg/mL | Tmax (hrs) | Half-life (hrs) |
|---|---|---|---|---|
| Healthy Subjects (n=14) | ||||
| 50 mg | 4.9 (16%) | 0.62 (52%) | 2.9 (66%) | 5.52 (37%) |
| 200 mg | 18.9 (17%) | 1.76 (30%) | 3.5 (57%) | 5.53 (25%) |
| 400 mg | 36.4 (26%) | 2.82 (28%) | 4.3 (37%) | 7.29 (36%) |
| Patients with Hansen’s Disease (n=6) | ||||
| 400 mg | 46.4 (44.1%) | 3.44 (52.6%) | 5.7 (27%) | 6.86 (17%) |
Coadministration of THALOMID (thalidomide) with a high-fat meal causes minor (<10%) changes in the observed AUC and Cmax values; however, it causes an increase in Tmax to approximately 6 hours.
In human plasma, the geometric mean plasma protein binding was 55% and 66%, respectively, for (+)(R) and ()(S)-thalidomide. In a pharmacokinetic study of thalidomide in HIV-seropositive adult male subjects receiving thalidomide 100 mg/day, thalidomide was detectable in the semen.
In a 14C-radiolabel ADME study in humans, unchanged drug is the predominant circulating component. Thalidomide is not a substrate of the cytochrome P450 system. At therapeutic concentrations, thalidomide is not an inhibitor or inducer of human cytochrome P450 enzymes in vitro. Pharmacokinetic drug-drug interactions with substrates, inhibitors or inducers of CYP450 are not anticipated.
The mean elimination half-life of thalidomide in plasma following single oral doses between 50 mg and 400 mg was 5.5 to 7.3 hours. Following a single 400 mg oral dose of radiolabeled thalidomide, the total mean recovery was 93.6% of the administered dose by Day 8. The majority of the radioactive dose was excreted within 48 hours following dose administration. In humans, 14C-thalidomide is primarily excreted in urine (91.9% of the radioactive dose) mainly as hydrolytic metabolites while fecal excretion is minor (<2% of the dose). Unchanged thalidomide is not eliminated by the kidney to a notable degree (<3.5% of the dose).
There is a linear relationship between body weight and estimated thalidomide clearance. In MM patients with body weight from 47-133 kg, thalidomide clearance ranged from approximately 6-12 L/h, representing an increase in thalidomide clearance of 0.605 L/h per 10 kg body weight increase.
Analysis of the data from pharmacokinetic studies in healthy volunteers and patients with Hansen’s disease ranging in age from 20 to 69 years does not reveal any age-related changes.
While a comparative trial of the effects of gender on thalidomide pharmacokinetics has not been conducted, examination of the data for thalidomide does not reveal any significant gender differences in pharmacokinetic parameter values.
Pharmacokinetic differences due to race have not been studied.
There is no apparent significant difference in measured pharmacokinetic parameter values between healthy human subjects and HIV-seropositive subjects following single-dose administration of THALOMID Capsules.
Analysis of data from a small study in Hansen’s patients suggests that these patients, relative to healthy subjects, may have an increased bioavailability of THALOMID. The increase is reflected both in an increased area under the curve and in increased peak plasma levels. The clinical significance of this increase is unknown.
No pharmacokinetic data are available in subjects below the age of 18 years.
Renal impairment is not expected to influence drug exposure since <3.5% of the dose is excreted in the urine as unchanged drug.
No clinical studies have been conducted in patients with hepatic impairment.
Two-year carcinogenicity studies were conducted in male and female rats and mice. No compound-related tumorigenic effects were observed at the highest dose levels of 3,000 mg/kg/day to male and female mice (38-fold greater than the highest recommended daily human dose of 400 mg based upon body surface area [BSA]), 3,000 mg/kg/day to female rats (75-fold the maximum human dose based upon BSA), and 300 mg/kg/day to male rats (7.5-fold the maximum human dose based upon BSA).
Thalidomide was neither mutagenic nor genotoxic in the following assays: the Ames bacterial (S. typhimurium and E. coli) reverse mutation assay, a Chinese hamster ovary cell (AS52/XPRT) forward mutation assay, and an in vivo mouse micronucleus test.
Fertility studies were conducted in male and female rabbits; no compound-related effects in mating and fertility indices were observed at any oral thalidomide dose level including the highest of 100 mg/kg/day to female rabbits and 500 mg/kg/day to male rabbits (approximately 5- and 25- fold the maximum human dose, respectively, based upon BSA). Testicular pathological and histopathological effects (classified as slight) were seen in male rabbits at dose levels ≥30 mg/kg/day (approximately 1.5-fold the maximum human dose based upon BSA).
The efficacy and safety of THALOMID in patients with multiple myeloma were evaluated in two randomized, multi-center studies (Study 1 and Study 2). Study 1 was an open-label study which randomized 207 symptomatic patients with newly diagnosed MM to THALOMID plus dexamethasone (N = 103) versus dexamethasone alone (N=104). The THALOMID dose was 200 mg daily and the dexamethasone dose was 40 mg orally once daily on days 1-4, 9-12, and 17-20 every 28-days. Each group was treated for four 28-day cycles.
Study 2 randomized 470 newly diagnosed patients with MM to THALOMID plus dexamethasone (N=235) versus placebo plus dexamethasone (N=235). In the THALOMID/dexamethasone arm, a starting dose of thalidomide 50 mg was escalated to 200 mg/day (cycle 2) once daily for 28 days. Patients in both treatment groups took 40 mg of dexamethasone once daily given on days 1-4, 9-12, and 17-20 (every 28 days). Beginning with Cycle 5, the dose of dexamethasone was reduced to 40 mg once daily on Days 1 to 4 of each cycle. Treatment continued as tolerated until disease progression.
Baseline demographics for both studies are presented in Table 6 and disease characteristics for the study population are summarized in Tables 7 (Study 1) and 8 (Study 2).
Table 6. Baseline Patient Demographics:
| Characteristic | Study 1 | Study 2 | ||
|---|---|---|---|---|
| THALOMID/Dexamethasone (N=103) | Dexamethasone (N=104) | THALOMID/Dexamethasone (N=235) | Placebo/Dexamethasone (N=235) | |
| Age (years) | ||||
| Median | 65 | 68 | 65 | 66 |
| Range | 37 – 83 | 38 – 83 | 39 – 86 | 31 – 84 |
| Gender*, N (%) | ||||
| Male | 53 (51) | 61 (59) | 118 (50) | 120 (51) |
| Female | 50 (49) | 42 (40) | 117 (50) | 115 (49) |
| Race†, N (%) | ||||
| Caucasian | 90 (87) | 90 (87) | 224 (95) | 221 (94) |
| Black | 11 (11) | 11 (11) | 7 (3) | 10 (4) |
| Other | 1 (1) | 2 (2) | 4 (2)‡ | 4 (2)§ |
* Missing information in Study 1 for 1 patient in the Dex alone group
† Missing information in Study 1 for 1 patient per arm
‡ Black/Hispanic [1 (0.4%)], Hispanic [2 (0.9%)], Hispanic/White [1 (0.4%)], Other [0 (0.0%)]
§ Hispanic [1 (0.4%)], Asian/Pacific Islander [2 (0.9%)], Other [1 (0.4%)]
Table 7. Baseline Disease Characteristics (Study 1):
| Disease Characteristic | THALOMID/Dexamethasone (N=103) | Dexamethasone alone (N=104) |
|---|---|---|
| Stage (Durie-Salmon), N (%)* | ||
| I | 14 (13.6%) | 17 (16.3%) |
| II | 47 (45.6%) | 44 (42.3%) |
| III | 41 (39.8%) | 43 (41.3%) |
| Immunoglobulin Type, N (%)† | ||
| IgA | 21 (20.4%) | 22 (21.2%) |
| IgG | 63 (61.2%) | 60 (57.7%) |
| IgM | 0 (0.0%) | 1 (1.0%) |
| Biclonal | 0 (0.0%) | 1 (1.0%) |
| Lytic Lesions‡ | ||
| None | 28 (27.1%) | 14 (13.5%) |
| 1-3 lesions | 24 (23.3%) | 19 (18.3%) |
| >3 lesions | 34 (33.0%) | 41 (39.4%) |
| Serum Light Chain§ | ||
| Kappa | 59 (57.3%) | 53 (51.0%) |
| Lambda | 28 (27.2%) | 40 (38.5%) |
* Missing information for 1 patient in Thal + Dex arm
† Missing information for 19 patients in Thal + Dex arm and 20 patients in Dex alone arm
‡ Missing information for 17 patients in Thal + Dex arm and 30 patients in Dex alone arm
§ Missing information for 16 patients in Thal + Dex arm and 11 patients in Dex alone arm
Table 8. Baseline Disease Characteristics (Study 2):
| Disease Characteristic | THALOMID/Dexamethasone (N=235) | Placebo/Dexamethasone (N=235) |
|---|---|---|
| Baseline MM Stage (Durie-Salmon), n (%) | ||
| I | 2 (1) | 2 (1) |
| II | 76 (32) | 88 (37) |
| III | 157 (69) | 145 (62) |
| ECOG Performance Status, n (%) | ||
| 0 | 40 (17) | 54 (23) |
| 1 | 124 (53) | 112 (48) |
| 2 | 70 (30) | 68 (29) |
| 3 | 0 (0) | 1 (<1) |
| Missing | 1 (<1) | 0 (0) |
| Lytic Bone Lesions, n (%) | ||
| Present | 185 (79) | 188 (80) |
| Absent | 49 (21) | 46 (20) |
| Missing | 1 (<1) | 1 (<1) |
| Bone Marrow Aspirate/Biopsy Cellularity, n (%) | ||
| Normal | 102 (43) | 108 (46) |
| Hyperplasia | 77 (33) | 76 (32) |
| Hypoplasia | 53 (23) | 50 (21) |
| Missing | 3 (1) | 1 (<1) |
| Baseline β-2 Microglobulin, n (%) | ||
| ≤2.5 mg/L | 33 (14) | 35 (15) |
| >2.5 mg/L | 200 (85) | 199 (85) |
| Missing | 2 (1) | 1 (<1) |
KEY: ECOG=Eastern Cooperative Oncology Group
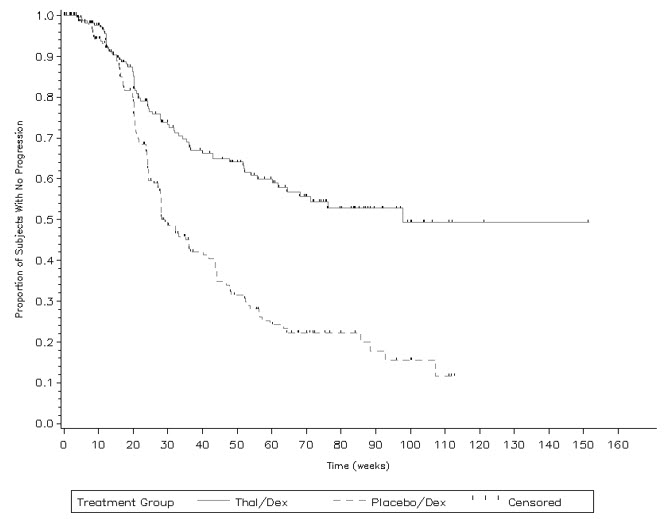
In Study 1, response rate was the primary endpoint. Response rates based on serum or urine paraprotein measurements were significantly higher in the combination arm (52% vs. 36%). The primary efficacy endpoint in Study 2 was time to progression (TTP), defined as the time from randomization to the first documentation of disease progression, based on the myeloma response criteria. A preplanned interim analysis for Study 2 demonstrated that the combination of THALOMID plus dexamethasone was superior to placebo plus dexamethasone with respect to TTP (Table 9).
Table 9. Summary of Efficacy (Study 2):
| Thalidomide/Dexamethasone (N=235) | Placebo/Dexamethasone (N=235) | |
|---|---|---|
| Time to Progression | ||
| Progressed – n (%) | 72 (31) | 126 (54) |
| Median (Weeks) (95% CI*) | 97.7 (61.86, NR) | 28.3 (27.71, 36.43) |
| Hazard Ratio (95% CI)† | 0.43 (0.32, 0.58) | |
| P-value‡ | <0.0001 | |
| Overall Survival | ||
| Death – n (%) | 57 (24) | 68 (29) |
| Median (Weeks) (95% CI*) | NR (112.14, NR) | 128.6 (113.43, NR) |
| Hazard Ratio (95% CI)† | 0.82 (0.57, 1.16) | |
| Myeloma Response Rate§ – n (%) | ||
| Complete Response (CR) | 18 (8) | 6 (3) |
| Partial Response (PR) | 130 (55) | 102 (43) |
| Overall Response (CR + PR) | 148 (63) | 108 (46) |
| 95% CI (%) | (56, 69) | (39, 53) |
* The 95% confidence intervals about the median overall TTP, or median overall survival. CI: confidence interval; NR: not reached.
† Based on a proportional hazards model comparing the hazard functions associated with treatment groups (thalidomide/dexamethasone:placebo/dexamethasone).
‡ P-value based on the interim analysis was compared with the nominal significance level of 0.0027. Based on a one-sided unstratified log rank test of survival curve differences between treatment groups.
§ Disease response assessments were determined according to the Bladé criteria. Response is the highest assessment of response during the treatment phase of the study.
The Kaplan-Meier plot of the time to progression by treatment group is presented in Figure 1.
Figure 1. Kaplan-Meier Plot of Time to Disease Progression:
KEY: Placebo/Dex=placebo/dexamethasone; Thal/Dex=THALOMID/dexamethasone
The primary data demonstrating the efficacy of thalidomide in the treatment of the cutaneous manifestations of moderate to severe ENL are derived from the published medical literature and from a retrospective study of 102 patients treated by the U.S. Public Health Service.
Two double-blind, randomized, controlled trials reported the dermatologic response to a 7-day course of 100 mg thalidomide (four times daily) or control. Dosage was lower for patients under 50 kg in weight.
Table 10. Double-Blind, Controlled Clinical Trials of Thalidomide in Patients with ENL: Cutaneous Response:
| Reference | No. of Patients | No. Treatment Courses* | Percent Responding** | |
|---|---|---|---|---|
| Iyer et al. Bull World Health Organization 1971;45:719 | 92 | 204 | Thalidomide 75% | Aspirin 25% |
| Sheskin et al. Int J Lep 1969;37:135 | 52 | 173 | Thalidomide 66% | Placebo 10% |
** Iyer: Complete response or lesions absent
** Sheskin: Complete improvement + “striking” improvement (i.e., >50% improvement)
* In patients with cutaneous lesions
Waters reported the results of two studies, both double-blind, randomized, placebo-controlled, crossover trials in a total of 10 hospitalized, steroid-dependent patients with chronic ENL treated with 100 mg thalidomide or placebo (three times daily). All patients also received dapsone. The primary endpoint was reduction in weekly steroid dosage.
Table 11. Double-Blind, Controlled Trial of Thalidomide in Patients with ENL: Reduction in Steroid Dosage:
| Reference | Duration of Treatment | No. of Patients | Number Responding | |
|---|---|---|---|---|
| Thalidomide | Placebo | |||
| Waters | 4 weeks | 9 | 4/5 | 0/4 |
| Lep Rev 1971;42:26 | 6 weeks (crossover) | 8 | 8/8 | 1/8 |
Data on the efficacy of thalidomide in prevention of ENL relapse were derived from a retrospective evaluation of 102 patients treated under the auspices of the U.S. Public Health Service. A subset of patients with ENL controlled on thalidomide demonstrated repeated relapse upon drug withdrawal and remission with reinstitution of therapy.
Twenty U.S. patients between the ages of 11 and 17 years were treated with thalidomide, generally at 100 mg daily. Response rates and safety profiles were similar to that observed in the adult population.
Thirty-two other published studies containing over 1600 patients consistently report generally successful treatment of the cutaneous manifestations of moderate to severe ENL with thalidomide.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.