TRINTELLIX Film-coated tablet Ref.[11067] Active ingredients: Vortioxetine
Source: FDA, National Drug Code (US) Revision Year: 2021
12.1. Mechanism of Action
The mechanism of the antidepressant effect of vortioxetine is not fully understood, but is thought to be related to its enhancement of serotonergic activity in the CNS through inhibition of the reuptake of serotonin (5-HT). It also has several other activities including 5-HT3 receptor antagonism and 5-HT1A receptor agonism. The contribution of these activities to vortioxetine's antidepressant effect has not been established.
12.2. Pharmacodynamics
Vortioxetine binds with high affinity to the human serotonin transporter (Ki=1.6 nM), but not to the norepinephrine (Ki=113 nM) or dopamine (Ki>1000 nM) transporters. Vortioxetine potently and selectively inhibits reuptake of serotonin (IC50=5.4 nM). Vortioxetine binds to 5-HT3 (Ki=3.7 nM), 5-HT1A (Ki=15 nM), 5-HT7 (Ki=19 nM), 5-HT1D (Ki=54 nM), and 5-HT1B (Ki=33 nM), receptors and is a 5-HT3, 5-HT1D, and 5-HT7 receptor antagonist, 5-HT1B receptor partial agonist, and 5-HT1A receptor agonist.
In humans, the mean 5-HT transporter occupancy, based on the results from two clinical PET studies using 5-HTT ligands ([11C]-MADAM or [11C]-DASB), was approximately 50% at 5 mg/day, 65% at 10 mg/day and approximately 80% at 20 mg/day in the regions of interest.
Effect on Cardiac Repolarization
The effect of vortioxetine 10 mg and 40 mg administered once daily on QTc interval was evaluated in a randomized, double-blind, placebo-, and active-controlled (moxifloxacin 400 mg), four-treatment-arm parallel study in 340 male subjects. In the study the upper bound of the one-sided 95% confidence interval for the QTc was below 10 ms, the threshold for regulatory concern. The oral dose of 40 mg is sufficient to assess the effect of metabolic inhibition.
Effect on Driving Performance
In a clinical study in healthy subjects, TRINTELLIX did not impair driving performance, or have adverse psychomotor or cognitive effects following single and multiple doses of 10 mg/day.
12.3. Pharmacokinetics
Vortioxetine pharmacological activity is due to the parent drug. The pharmacokinetics of vortioxetine (2.5 mg to 60 mg) are linear and dose-proportional when vortioxetine is administered once daily. The mean terminal half-life is approximately 66 hours, and steady-state plasma concentrations are typically achieved within two weeks of dosing.
Absorption
The maximal plasma vortioxetine concentration (Cmax) after dosing is reached within 7 to 11 hours postdose (Tmax). Steady-state mean Cmax values were 9, 18, and 33 ng/mL following doses of 5, 10, and 20 mg/day. Absolute bioavailability is 75%.
Effect of Food
No effect of food on the pharmacokinetics was observed.
Distribution
The apparent volume of distribution of vortioxetine is approximately 2600 L, indicating extensive extravascular distribution. The plasma protein binding of vortioxetine in humans is 98%, independent of plasma concentrations. No apparent difference in the plasma protein binding between healthy subjects and subjects with hepatic (mild, moderate or severe) or renal (mild, moderate, severe, ESRD) impairment is observed.
Elimination
Metabolism
Vortioxetine is extensively metabolized primarily through oxidation via cytochrome P450 isozymes CYP2D6, CYP3A4/5, CYP2C19, CYP2C9, CYP2A6, CYP2C8 and CYP2B6 and subsequent glucuronic acid conjugation. CYP2D6 is the primary enzyme catalyzing the metabolism of vortioxetine to its major, pharmacologically inactive, carboxylic acid metabolite, and poor metabolizers of CYP2D6 have approximately twice the vortioxetine plasma concentration of extensive metabolizers [see Dosage and Administration (2.5)].
Excretion
Following a single oral dose of [14C]-labeled vortioxetine, approximately 59% and 26% of the administered radioactivity was recovered in the urine and feces, respectively as metabolites. Negligible amounts of unchanged vortioxetine were excreted in the urine up to 48 hours. The presence of hepatic (mild, moderate or severe) or renal impairment (mild, moderate, severe and ESRD) did not affect the apparent clearance of vortioxetine.
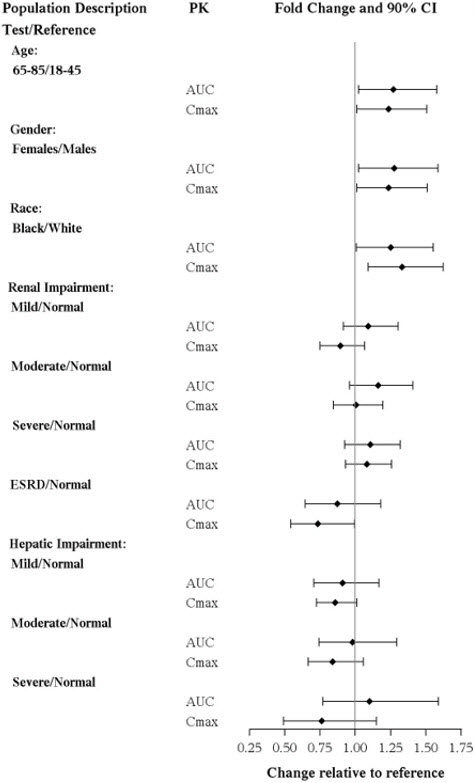
Specific Populations
No clinically significant differences in the exposures of vortioxetine were observed based on age, gender, ethnicity, renal function, or hepatic function.
The effects of intrinsic patient factors on the pharmacokinetics of vortioxetine are presented in Figure 1.
Figure 1. Impact of Intrinsic Factors on Vortioxetine PK:
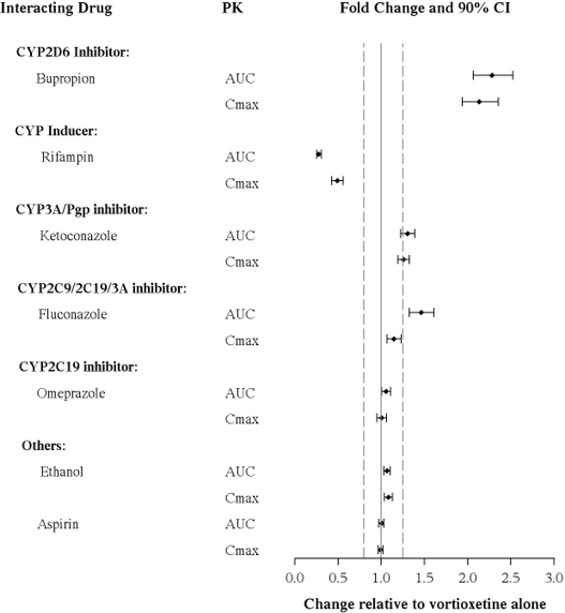
Drug Interaction Studies
Clinical Studies
Other Drugs on TRINTELLIX:
The effects of other drugs on vortioxetine exposure are summarized in Figure 2.
Figure 2. Impact of Other Drugs on Vortioxetine PK:
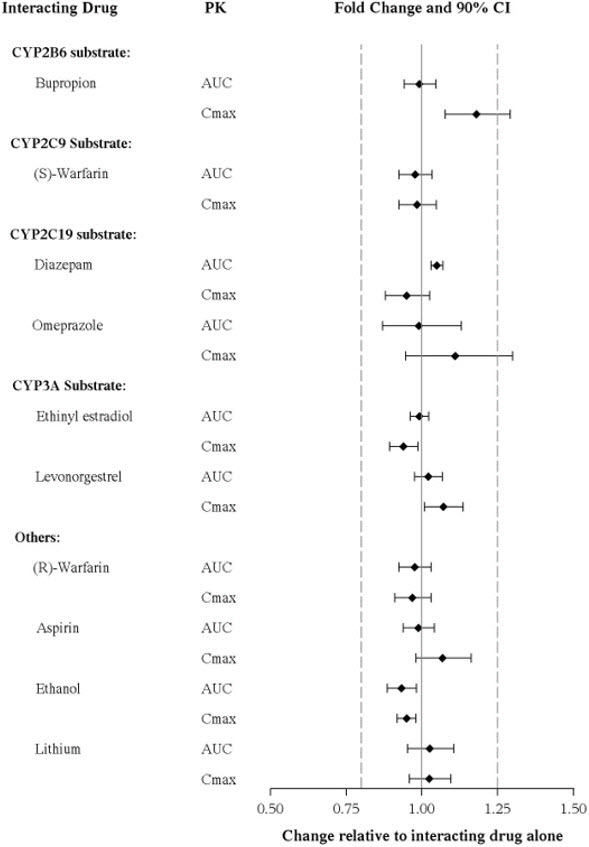
TRINTELLIX on Other Drugs:
The effects of vortioxetine on the exposures of other drugs are summarized in Figure 3.
Figure 3. Impact of Vortioxetine on PK of Other Drugs:
In Vitro
Vortioxetine and its metabolite(s) are unlikely to inhibit the following CYP enzymes and transporter based on in vitro data: CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, CYP2E1, CYP3A4/5, P-gp, BCRP, BSEP, MATE1, MATE2-K, OAT1, OAT3, OATP1B1, OATP1B3, OCT1 and OCT2. As such, no clinically relevant interactions with drugs metabolized/transported by these CYP enzymes or transporters would be expected.
In addition, vortioxetine did not induce CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, and CYP3A4/5 in an in vitro study in cultured human hepatocytes. Chronic administration of TRINTELLIX is unlikely to induce the metabolism of drugs metabolized by these CYP isoforms. Furthermore, in a series of clinical drug interaction studies, coadministration of TRINTELLIX with substrates for CYP2B6 (e.g., bupropion), CYP2C9 (e.g., warfarin), and CYP2C19 (e.g., diazepam), had no clinical meaningful effect on the pharmacokinetics of these substrates.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Carcinogenicity studies were conducted in which CD-1 mice and Wistar rats were given oral doses of vortioxetine up to 50 and 100 mg/kg/day for male and female mice, respectively, and 40 and 80 mg/kg/day for male and female rats, respectively, for two years. The doses in the two species were approximately 12, 24, 20, and 39 times, respectively, the maximum recommended human dose (MRHD) of 20 mg on a mg/m² basis.
In rats, the incidence of benign polypoid adenomas of the rectum was statistically significantly increased in females at doses 39 times the MRHD, but not at 15 times the MRHD. These were considered related to inflammation and hyperplasia and possibly caused by an interaction with a vehicle component of the formulation used for the study. The finding did not occur in male rats at 20 times the MRHD.
In mice, vortioxetine was not carcinogenic in males or females at doses up to 12 and 24 times, respectively, the MRHD.
Mutagenicity
Vortioxetine was not genotoxic in the in vitro bacterial reverse mutation assay (Ames test), an in vitro chromosome aberration assay in cultured human lymphocytes, and an in vivo rat bone marrow micronucleus assay.
Impairment of Fertility
Treatment of rats with vortioxetine at doses up to 120 mg/kg/day had no effect on male or female fertility, which is 58 times the maximum recommended human dose (MRHD) of 20 mg on a mg/m² basis.
14. Clinical Studies
The efficacy of TRINTELLIX in treatment for MDD was established in six, 6 to 8 week randomized, double-blind, placebo-controlled, fixed-dose studies (including one study in the elderly) and one maintenance study in adult inpatients and outpatients who met the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) criteria for MDD.
Adults (aged 18 years to 75 years)
The efficacy of TRINTELLIX in patients aged 18 years to 75 years was demonstrated in five, 6 to 8 week, placebo-controlled studies (Studies 1 to 5 in Table 5). In these studies, patients were randomized to TRINTELLIX 5 mg, 10 mg, 15 mg or 20 mg or placebo once daily. For patients who were randomized to TRINTELLIX 15 mg/day or 20 mg/day, the final doses were titrated up from 10 mg/day after the first week.
The primary efficacy measures were the Hamilton Depression Scale (HAMD-24) total score in Study 2 and the Montgomery-Asberg Depression Rating Scale (MADRS) total score in all other studies. In each of these studies, at least one dose group of TRINTELLIX was superior to placebo in improvement of depressive symptoms as measured by mean change from baseline to endpoint visit on the primary efficacy measurement (see Table 5). Subgroup analysis by age, gender or race did not suggest any clear evidence of differential responsiveness. Two studies of the 5 mg dose in the U.S. (not represented in Table 5) failed to show effectiveness.
Elderly Study (aged 64 years to 88 years)
The efficacy of TRINTELLIX for the treatment of MDD was also demonstrated in a randomized, double-blind, placebo-controlled, fixed-dose study of TRINTELLIX in elderly patients (aged 64 years to 88 years) with MDD (Study 6 in Table 5). Patients meeting the diagnostic criteria for recurrent MDD with at least one previous major depressive episode before the age of 60 years and without comorbid cognitive impairment (Mini Mental State Examination score <24) received TRINTELLIX 5 mg or placebo.
Table 5. Primary Efficacy Results of 6 Week to 8 Week Clinical Trials:
| Study No. [Primary Measure] | Treatment Group | Number of Patients | Mean Baseline Score (SD) | LS Mean Change from Baseline (SE) | Placebo-subtracted Difference* (95% CI) |
|---|---|---|---|---|---|
| Study 1 [MADRS] Non-US Study | TRINTELLIX (5 mg/day)† | 108 | 34.1 (2.6) | -20.4 (1.0) | -5.9 (-8.6, -3.2) |
| TRINTELLIX (10 mg/day)† | 100 | 34.0 (2.8) | -20.2 (1.0) | -5.7 (-8.5, -2.9) | |
| Placebo | 105 | 33.9 (2.7) | -14.5 (1.0) | -- | |
| Study 2 [HAMD-24] Non-US Study | TRINTELLIX (5 mg/day) | 139 | 32.2 (5.0) | -15.4 (0.7) | -4.1 (-6.2, -2.1) |
| TRINTELLIX (10 mg/day)† | 139 | 33.1 (4.8) | -16.2 (0.8) | -4.9 (-7.0, -2.9) | |
| Placebo | 139 | 32.7 (4.4) | -11.3 (0.7) | -- | |
| Study 3 [MADRS] Non-US Study | TRINTELLIX (15 mg/day) ?footnoteRef? | 149 | 31.8 (3.4) | -17.2 (0.8) | -5.5 (-7.7, -3.4) |
| TRINTELLIX (20 mg/day)† | 151 | 31.2 (3.4) | -18.8 (0.8) | -7.1 (-9.2, -5.0) | |
| Placebo | 158 | 31.5 (3.6) | -11.7 (0.8) | -- | |
| Study 4 [MADRS] US Study | TRINTELLIX (15 mg/day) | 145 | 31.9 (4.1) | -14.3 (0.9) | -1.5 (-3.9, 0.9) |
| TRINTELLIX (20 mg/day)† | 147 | 32.0 (4.4) | -15.6 (0.9) | -2.8 (-5.1, -0.4) | |
| Placebo | 153 | 31.5 (4.2) | -12.8 (0.8) | -- | |
| Study 5 [MADRS] US Study | TRINTELLIX (10 mg/day) | 154 | 32.2 (4.5) | -13.0 (0.8) | -2.2 (-4.5, 0.1) |
| TRINTELLIX (20 mg/day)† | 148 | 32.5 (4.3) | -14.4 (0.9) | -3.6 (-5.9, -1.4) | |
| Placebo | 155 | 32.0 (4.0) | -10.8 (0.8) | -- | |
| Study 6 (elderly) [HAMD-24] US and Non-US | TRINTELLIX (5 mg/day)† | 155 | 29.2 (5.0) | -13.7 (0.7) | -3.3 (-5.3, -1.3) |
| Placebo | 145 | 29.4 (5.1) | -10.3 (0.8) | -- |
SD: standard deviation; SE: standard error; LS Mean: least-squares mean; CI: unadjusted confidence interval.
* Difference (drug minus placebo) in least-squares mean change from baseline.
† Doses that are statistically significantly superior to placebo after adjusting for multiplicity.
TRINTELLIX was superior to placebo on the Clinical Global Impression of Improvement (CGI-I) scale, which is a clinician's impression of how much the patient's clinical condition has improved or worsened relative to baseline on a scale of 1 (very much improved) to 7 (very much worse).
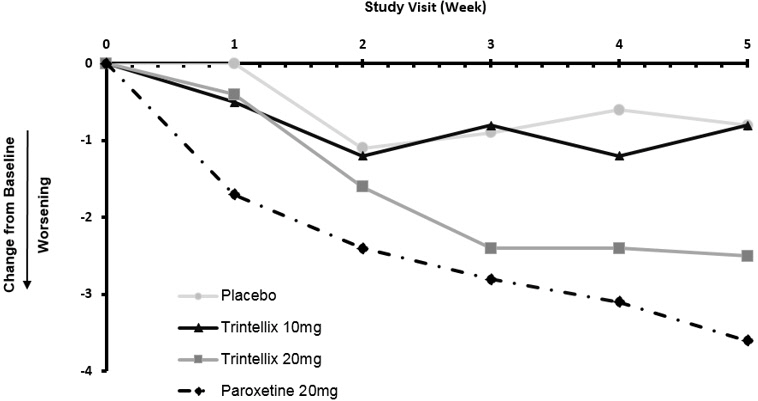
Time Course of Treatment Response
In the 6 to 8 week placebo-controlled studies, an effect of TRINTELLIX based on the primary efficacy measure was generally observed starting at Week 2 and increased in subsequent weeks with the full antidepressant effect of TRINTELLIX generally not seen until Study Week 4 or later. Figure 4 depicts time course of response in U.S. based on the primary efficacy measure (MADRS) in Study 5.
Figure 4. Change from Baseline in MADRS Total Score by Study Visit (Week) in Study 5:
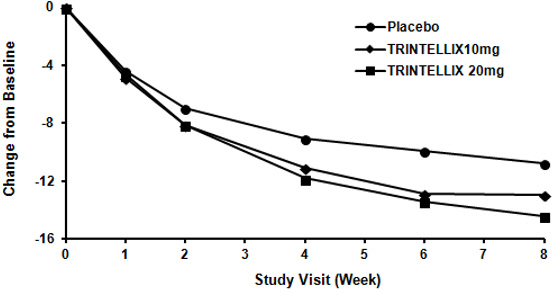
Figure 5. Difference from Placebo in Mean Change from Baseline in MADRS Total Score at Week 6 or Week 8:
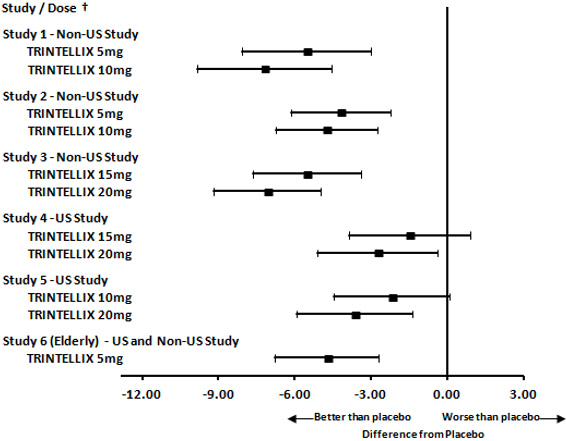
† Results (point estimate and unadjusted 95% confidence interval) are from mixed model for repeated measures (MMRM) analysis. In Studies 1 and 6, the primary analysis was not based on MMRM and in Studies 2 and 6 the primary efficacy measure was not based on MADRS
Digit Symbol Substitution Test in Major Depressive Disorder
Two, eight week, randomized, double-blind, placebo-controlled studies were conducted to evaluate the effect of TRINTELLIX on the Digit Symbol Substitution Test (DSST) during the treatment of acute MDD. The DSST is a neuropsychological test that most specifically measures processing speed, an aspect of cognitive function that may be impaired in MDD. Patients are asked to match nine symbols with their corresponding number (1 to 9) according to a key; the score is the correct number of matches achieved in 90 seconds. For reference, the mean score for healthy 45 to 54 year-old subjects is 50 (SD=15).
Study 7 randomized adult patients meeting the diagnostic criteria for recurrent MDD to receive TRINTELLIX 10 mg, TRINTELLIX 20 mg, or placebo once daily. Study 8 randomized adult patients meeting the diagnostic criteria for recurrent MDD and reporting subjective difficulty concentrating or slow thinking to receive a flexible dose of TRINTELLIX (10 or 20 mg) or placebo once daily. Neither study included patients whose MDD was in remission yet who continued to experience difficulty concentrating or slow thinking. Patients' mean age was 46 (SD=12) and 45 (SD=12) in Study 7 and 8, respectively. In both studies, patients in the TRINTELLIX group had a statistically significantly greater improvement in number of correct responses on the DSST (Table 6); depressed mood as assessed by change from baseline in MADRS total score also improved in both studies.
Table 6. Effect of TRINTELLIX on the Digit Symbol Substitution Test (DSST):
| Study No. | Treatment Group | Number of Patients | Mean Baseline Score (SD) | LS Mean Change from Baseline (SE) | Placebo-subtracted Difference* (95% CI) |
|---|---|---|---|---|---|
| Study 7 | TRINTELLIX (10 mg/day)† | 193 | 42.0 (12.6) | 9.0 (0.6) | 4.2 (2.5, 5.9) |
| TRINTELLIX (20 mg/day)† | 204 | 41.6 (12.7) | 9.1 (0.6) | 4.3 (2.6, 5.9) | |
| Placebo | 194 | 42.4 (13.8) | 4.8 (0.6) | -- | |
| Study 8 | TRINTELLIX (10/20 mg/day)† | 175 | 42.1 (11.9) | 4.6 (0.5) | 1.8 (0.3, 3.2) |
| Placebo | 167 | 43.0 (12.3) | 2.9 (0.5) | -- |
SD: standard deviation; SE: standard error; LS Mean: least-squares mean; CI: unadjusted confidence interval.
* Difference (drug minus placebo) in least-squares mean change from baseline.
† Doses are statistically significantly superior to placebo.
The effects observed on DSST may reflect improvement in depression. Comparative studies have not been conducted to demonstrate a therapeutic advantage over other antidepressants on the DSST.
Maintenance Studies
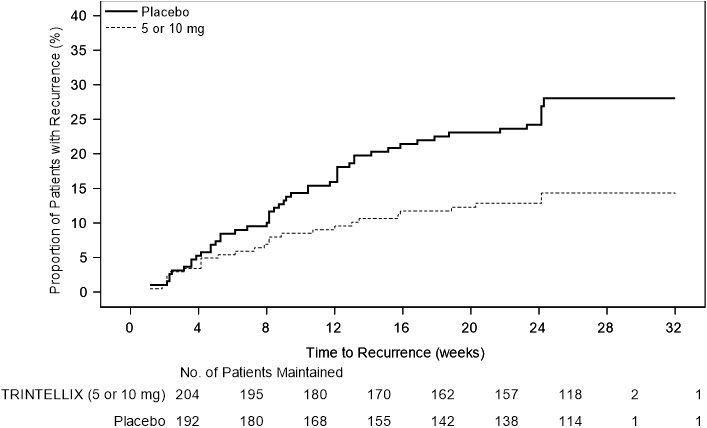
In a non-U.S. maintenance study (Study 9 in Figure 6), 639 patients meeting DSM-IV-TR criteria for MDD received flexible doses of TRINTELLIX (5 mg or 10 mg) once daily during an initial 12 week open-label treatment phase; the dose of TRINTELLIX was fixed during Weeks 8 to 12. Three hundred ninety six (396) patients who were in remission (MADRS total score ≤10 at both Weeks 10 and 12) after open-label treatment were randomly assigned to continuation of a fixed dose of TRINTELLIX at the final dose they responded to (about 75% of patients were on 10 mg/day) during the open-label phase or to placebo for 24 to 64 weeks. Approximately 61% of randomized patients satisfied remission criterion (MADRS total score ≤10) for at least four weeks (since Week 8), and 15% for at least eight weeks (since Week 4). Patients on TRINTELLIX experienced a statistically significantly longer time to have recurrence of depressive episodes than did patients on placebo. Recurrence of depressive episode was defined as a MADRS total score ≥22 or lack of efficacy as judged by the investigator.
Figure 6. Kaplan-Meier Estimates of Proportion of Patients with Recurrence (Study 9):
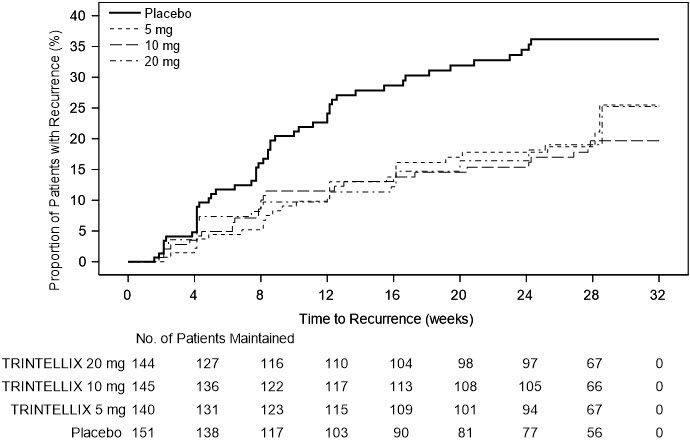
In a U.S.-based maintenance study (Study 10 in Figure 7), 1106 patients meeting DSM-IV-TR criteria for MDD were treated with a fixed dose of TRINTELLIX 10 mg once daily during an initial 16 week open-label treatment phase. Five hundred and eighty (580) patients who were in remission (MADRS total score ≤12 at both Weeks 14 and 16) after open-label treatment were randomized in a 1:1:1:1 ratio to TRINTELLIX 5 mg/day, 10 mg/day, 20 mg/day, or placebo daily for 32 weeks. The definition of recurrence of depressive episodes was the same as for Study 9. For all three doses of TRINTELLIX evaluated, patients treated with TRINTELLIX experienced a statistically significantly longer time to recurrence of depressive episodes than did patients treated with placebo.
Figure 7. Kaplan-Meier Estimates of Proportion of Patients with Recurrence (Study 10):
Prospective Evaluation of Treatment Emergent Sexual Dysfunction (TESD)
Two, randomized, double-blind, active-controlled studies were conducted to prospectively compare the incidence of TESD between TRINTELLIX and SSRIs via a validated self-rated measure of sexual function, the Changes in Sexual Functioning Questionnaire Short Form (CSFQ-14). The CSFQ-14 is designed to measure illness- and medication-related changes in sexual functioning that consists of 14 items measuring sexual functioning as a total score. The CSFQ-14 consists of subscales that assess the three phases of the sexual response cycle (desire, arousal, and orgasm). Higher scores on the CSFQ-14 indicate greater sexual function and for reference, a 2-3 point change is considered clinically meaningful.
Effect of Switching from SSRI to TRINTELLIX on TESD
The effect of TRINTELLIX on TESD induced by prior SSRI treatment in MDD patients whose depressive symptoms were adequately treated was evaluated in an eight-week, randomized, double-blind, active-controlled (escitalopram), flexible-dose study (Study 11). Patients taking citalopram, sertraline, or paroxetine for at least eight weeks duration and who were experiencing sexual dysfunction attributed to their SSRI treatment were switched to TRINTELLIX (n=217) or escitalopram (n=207). For both TRINTELLIX and escitalopram, patients were started on 10 mg, increased to 20 mg at Week 1, followed by flexible dosing. The majority of subjects received the 20 mg dose of TRINTELLIX (65.6%) or the 20 mg dose of escitalopram (71.9%) during the study.
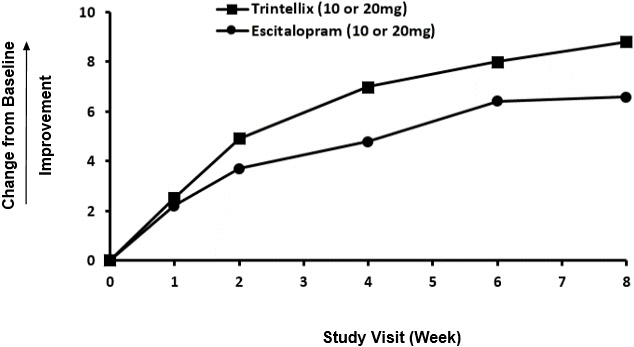
Improvement in TESD induced by prior SSRI treatment in subjects switched to TRINTELLIX was superior to the improvement observed in those subjects who switched to escitalopram (2.2 point improvement vs escitalopram on the change from Baseline in CSFQ-14 total score, with 95% confidence interval 0.48–4.02), after eight weeks of treatment, while both drugs maintained the subjects' prior antidepressant response. For change from Baseline in CSFQ-14, see Figure 8.
Figure 8. Change from Baseline in CSFQ-14 Total Score by Study Visit (Week) in Study 11:
Effects in Healthy Volunteers with Normal Sexual Functioning at Baseline
In a randomized Healthy Volunteer study (Study 12) with 348 subjects aged 18 years to 40 years with normal sexual functioning without the confounding effect of depression, TESD with TRINTELLIX 10 mg (n=85), but not with TRINTELLIX 20 mg (n=91), was statistically significantly less than with paroxetine 20 mg (n=83) [see Adverse Reactions (6.1)]. Paroxetine 20 mg was statistically significantly worse than placebo (n=89), confirming assay sensitivity in this study. For change from Baseline in CSFQ-14, see Figure 9.
Figure 9. Change from Baseline in CSFQ-14 Total Score by Study Visit (Week) in Healthy Volunteers (Study 12):
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.