VYVANSE Capsule / Tablet chewable Ref.[11110] Active ingredients: Lisdexamfetamine
Source: FDA, National Drug Code (US) Revision Year: 2019
12.1. Mechanism of Action
Lisdexamfetamine is a prodrug of dextroamphetamine. Amphetamines are non-catecholamine sympathomimetic amines with CNS stimulant activity. The exact mode of therapeutic action in ADHD and BED is not known.
12.2. Pharmacodynamics
Amphetamines block the reuptake of norepinephrine and dopamine into the presynaptic neuron and increase the release of these monoamines into the extraneuronal space. The parent drug, lisdexamfetamine, does not bind to the sites responsible for the reuptake of norepinephrine and dopamine in vitro.
12.3. Pharmacokinetics
Pharmacokinetic studies after oral administration of lisdexamfetamine dimesylate have been conducted in healthy adult (capsule and chewable tablet formulations) and pediatric (6 to 12 years) patients with ADHD (capsule formulation). After single dose administration of lisdexamfetamine dimesylate, pharmacokinetics of dextroamphetamine was found to be linear between 30 mg and 70 mg in a pediatric study, and between 50 mg and 250 mg in an adult study. Dextroamphetamine pharmacokinetic parameters following administration of lisdexamfetamine dimesylate in adults exhibited low inter-subject (<25%) and intra-subject (<8%) variability.
There is no accumulation of lisdexamfetamine and dextroamphetamine at steady state in healthy adults.
Safety and efficacy have not been studied above the maximum recommended dose of 70 mg.
Absorption
Capsule formulation
Following single-dose oral administration of VYVANSE capsule (30 mg, 50 mg, or 70 mg) in patients ages 6 to 12 years with ADHD under fasted conditions, Tmax of lisdexamfetamine and dextroamphetamine was reached at approximately 1 hour and 3.5 hour post dose, respectively. Weight/Dose normalized AUC and Cmax values were the same in pediatric patients ages 6 to 12 years as the adults following single doses of 30 mg to 70 mg VYVANSE capsule.
Food effect on capsule formulation
Neither food (a high fat meal or yogurt) nor orange juice affects the observed AUC and Cmax of dextroamphetamine in healthy adults after single-dose oral administration of 70 mg of VYVANSE capsules. Food prolongs Tmax by approximately 1 hour (from 3.8 hour at fasted state to 4.7 hour after a high fat meal or to 4.2 hour with yogurt). After an 8-hour fast, the AUC for dextroamphetamine following oral administration of lisdexamfetamine dimesylate in solution and as intact capsules were equivalent.
Chewable Tablet formulation
After a single dose administration of 60 mg VYVANSE chewable tablet in healthy subjects under fasted conditions, Tmax of lisdexamfetamine and dextroamphetamine was reached at approximately 1 hour and 4.4 hour post dose, respectively. Compared to 60 mg VYVANSE capsule, exposure (Cmax and AUC) to lisdexamfetamine was about 15% lower. The exposure (Cmax and AUCinf) of dextroamphetamine is similar between VYVANSE chewable tablet and VYVANSE capsule.
Food effect on tablet formulation
Administration of 60 mg VYVANSE chewable tablet with food (a high-fat meal) decreases the exposure (Cmax and AUCinf) of dextroamphetamine by about 5% to 7%, and prolongs mean Tmax by approximately 1 hour (from 3.9 hrs at fasted state to 4.9 hours).
Elimination
Plasma concentrations of unconverted lisdexamfetamine are low and transient, generally becoming non-quantifiable by 8 hours after administration. The plasma elimination half-life of lisdexamfetamine typically averaged less than one hour in studies of lisdexamfetamine dimesylate in volunteers. The mean plasma elimination half-life of dextroamphetamine was about 12 hours after oral administration of lisdexamfetamine dimesylate.
Metabolism
Lisdexamfetamine is converted to dextroamphetamine and l-lysine primarily in blood due to the hydrolytic activity of red blood cells after oral administration of lisdexamfetamine dimesylate. In vitro data demonstrated that red blood cells have a high capacity for metabolism of lisdexamfetamine; substantial hydrolysis occurred even at low hematocrit levels (33% of normal). Lisdexamfetamine is not metabolized by cytochrome P450 enzymes.
Excretion
Following oral administration of a 70 mg dose of radiolabeled lisdexamfetamine dimesylate to 6 healthy subjects, approximately 96% of the oral dose radioactivity was recovered in the urine and only 0.3% recovered in the feces over a period of 120 hours. Of the radioactivity recovered in the urine, 42% of the dose was related to amphetamine, 25% to hippuric acid, and 2% to intact lisdexamfetamine.
Specific Populations
Exposures of dextroamphetamine in specific populations are summarized in Figure 1.
Figure 1. Specific Populations*:
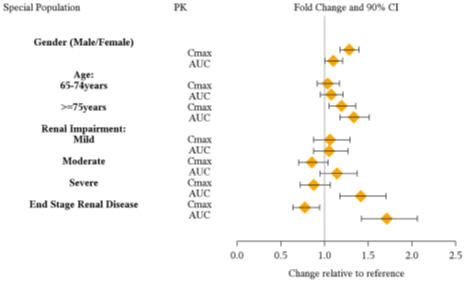
* Figure 1 shows the geometric mean ratios and the 90% confidence limits for Cmax and AUC of d-amphetamine. Comparison for gender uses males as the reference. Comparison for age uses 55-64 years as the reference.
Drug Interaction Studies
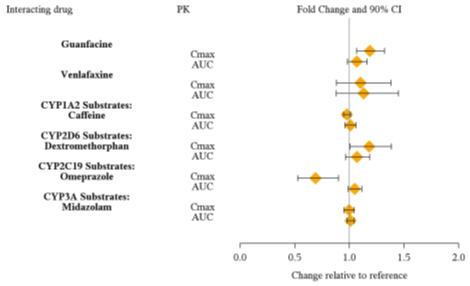
Effects of other drugs on the exposures of dextroamphetamine are summarized in Figure 2.
Figure 2. Effect of Other Drugs on VYVANSE:
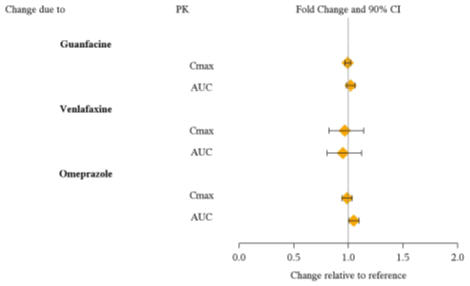
The effects of VYVANSE on the exposures of other drugs are summarized in Figure 3.
Figure 3. Effect of VYVANSE on Other Drugs:
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Carcinogenicity studies of lisdexamfetamine dimesylate have not been performed. No evidence of carcinogenicity was found in studies in which d-, l-amphetamine (enantiomer ratio of 1:1) was administered to mice and rats in the diet for 2 years at doses of up to 30 mg/kg/day in male mice, 19 mg/kg/day in female mice, and 5 mg/kg/day in male and female rats.
Mutagenesis
Lisdexamfetamine dimesylate was not clastogenic in the mouse bone marrow micronucleus test in vivo and was negative when tested in the E. coli and S. typhimurium components of the Ames test and in the L5178Y/TK+- mouse lymphoma assay in vitro.
Impairment of Fertility
Amphetamine (d- to l-enantiomer ratio of 3:1) did not adversely affect fertility or early embryonic development in the rat at doses of up to 20 mg/kg/day.
13.2. Animal Toxicology and/or Pharmacology
Acute administration of high doses of amphetamine (d- or d,l-) has been shown to produce long-lasting neurotoxic effects, including irreversible nerve fiber damage, in rodents. The significance of these findings to humans is unknown.
14. Clinical Studies
Efficacy of VYVANSE in the treatment of ADHD has been established in the following trials:
- Three short-term trials in children (6 to 12 years, Studies 1, 2, 3)
- One short-term trial in adolescents (13 to 17 years, Study 4)
- One short-term trial in children and adolescents (6 to 17 years, Study 5)
- Two short-term trials in adults (18 to 55 years, Studies 7, 8)
- Two randomized withdrawal trials in children and adolescents (6 to 17 years, Study 6), and adults (18 to 55 years, Study 9)
Efficacy of VYVANSE in the treatment of moderate to severe BED in adults has been established in the following trials:
- One randomized trial in adults (18 to 55 years, Study 10)
- Two short-term trials in adults (18 to 55 years, Studies 11 and 12)
- One randomized withdrawal study in adults (18 to 55 years, Study 13)
14.1 Attention Deficit Hyperactivity Disorder (ADHD)
Patients Ages 6 to 12 Years Old with ADHD
A double-blind, randomized, placebo-controlled, parallel-group study (Study 1) was conducted in children ages 6 to 12 years (N=290) who met DSM-IV criteria for ADHD (either the combined type or the hyperactive-impulsive type). Patients were randomized to receive final doses of 30 mg, 50 mg, or 70 mg of VYVANSE or placebo once daily in the morning for a total of four weeks of treatment. All patients receiving VYVANSE were initiated on 30 mg for the first week of treatment. Patients assigned to the 50 mg and 70 mg dose groups were titrated by 20 mg per week until they achieved their assigned dose. The primary efficacy outcome was change in Total Score from baseline to endpoint in investigator ratings on the ADHD Rating Scale (ADHD-RS), an 18-item questionnaire with a score range of 0-54 points that measures the core symptoms of ADHD which includes both hyperactive/impulsive and inattentive subscales. Endpoint was defined as the last post-randomization treatment week (i.e. Weeks 1 through 4) for which a valid score was obtained. All VYVANSE dose groups were superior to placebo in the primary efficacy outcome. Mean effects at all doses were similar; however, the highest dose (70 mg/day) was numerically superior to both lower doses (Study 1 in Table 7). The effects were maintained throughout the day based on parent ratings (Conners' Parent Rating Scale) in the morning (approximately 10 am), afternoon (approximately 2 pm), and early evening (approximately 6 pm).
A double-blind, placebo-controlled, randomized, crossover design, analog classroom study (Study 2) was conducted in children ages 6 to 12 years (N=52) who met DSM-IV criteria for ADHD (either the combined type or the hyperactive-impulsive type). Following a 3-week open-label dose optimization with Adderall XR , patients were randomly assigned to continue their optimized dose of Adderall XR (10 mg, 20 mg, or 30 mg), VYVANSE (30 mg, 50 mg, or 70 mg), or placebo once daily in the morning for 1 week each treatment. Efficacy assessments were conducted at 1, 2, 3, 4.5, 6, 8, 10, and 12 hours post-dose using the Swanson, Kotkin, Agler, M.Flynn, and Pelham Deportment scores (SKAMP-DS), a 4-item subscale of the SKAMP with scores ranging from 0 to 24 points that measures deportment problems leading to classroom disruptions. A significant difference in patient behavior, based upon the average of investigator ratings on the SKAMP-DS across the 8 assessments were observed between patients when they received VYVANSE compared to patients when they received placebo (Study 2 in Table 7). The drug effect reached statistical significance from hours 2 to 12 post-dose, but was not significant at 1 hour.
A second double-blind, placebo-controlled, randomized, crossover design, analog classroom study (Study 3) was conducted in children ages 6 to 12 years (N=129) who met DSM-IV criteria for ADHD (either the combined type or the hyperactive-impulsive type). Following a 4-week open-label dose optimization with VYVANSE (30 mg, 50 mg, 70 mg), patients were randomly assigned to continue their optimized dose of VYVANSE or placebo once daily in the morning for 1 week each treatment. A significant difference in patient behavior, based upon the average of investigator ratings on the SKAMP-Deportment scores across all 7 assessments conducted at 1.5, 2.5, 5.0, 7.5, 10.0, 12.0, and 13.0 hours post-dose, were observed between patients when they received VYVANSE compared to patients when they received placebo (Study 3 in Table 7, Figure 4).
Patients Ages 13 to 17 Years Old with ADHD
A double-blind, randomized, placebo-controlled, parallel-group study (Study 4) was conducted in adolescents ages 13 to 17 years (N=314) who met DSM-IV criteria for ADHD. In this study, patients were randomized in a 1:1:1:1 ratio to a daily morning dose of VYVANSE (30 mg/day, 50 mg/day or 70 mg/day) or placebo for a total of four weeks of treatment. All patients receiving VYVANSE were initiated on 30 mg for the first week of treatment. Patients assigned to the 50 mg and 70 mg dose groups were titrated by 20 mg per week until they achieved their assigned dose. The primary efficacy outcome was change in Total Score from baseline to endpoint in investigator ratings on the ADHD Rating Scale (ADHD-RS). Endpoint was defined as the last post-randomization treatment week (i.e. Weeks 1 through 4) for which a valid score was obtained. All VYVANSE dose groups were superior to placebo in the primary efficacy outcome (Study 4 in Table 7).
Patients Ages 6 to 17 Years Old: Short-Term Treatment in ADHD
A double-blind, randomized, placebo- and active-controlled parallel-group, dose-optimization study (Study 5) was conducted in children and adolescents ages 6 to 17 years (n=336) who met DSM-IV criteria for ADHD. In this eight-week study, patients were randomized to a daily morning dose of VYVANSE (30, 50 or 70mg/day), an active control, or placebo (1:1:1). The study consisted of a Screening and Washout Period (up to 42 days), a 7-week Double-blind Evaluation Period (consisting of a 4-week Dose-Optimization Period followed by a 3-week Dose-Maintenance Period), and a 1-week Washout and Follow-up Period. During the Dose Optimization Period, subjects were titrated until an optimal dose, based on tolerability and investigator's judgment, was reached. VYVANSE showed significantly greater efficacy than placebo. The placebo-adjusted mean reduction from baseline in the ADHD-RS-IV total score was 18.6. Subjects on VYVANSE also showed greater improvement on the Clinical Global Impression-Improvement (CGI-I) rating scale compared to subjects on placebo (Study 5 in Table 7).
Patients Ages 6 to 17 Years Old: Maintenance Treatment in ADHD
Maintenance of Efficacy Study (Study 6) - A double-blind, placebo-controlled, randomized withdrawal study was conducted in children and adolescents ages 6 to 17 (N=276) who met the diagnosis of ADHD (DSM-IV criteria). A total of 276 patients were enrolled into the study, 236 patients participated in Study 5 and 40 subjects directly enrolled. Subjects were treated with open-label VYVANSE for at least 26 weeks prior to being assessed for entry into the randomized withdrawal period. Eligible patients had to demonstrate treatment response as defined by CGI-S <3 and Total Score on the ADHD-RS ≤22. Patients that maintained treatment response for 2 weeks at the end of the open label treatment period were eligible to be randomized to ongoing treatment with the same dose of VYVANSE (N=78) or switched to placebo (N=79) during the double-blind phase. Patients were observed for relapse (treatment failure) during the 6 week double blind phase. A significantly lower proportion of treatment failures occurred among VYVANSE subjects (15.8%) compared to placebo (67.5%) at endpoint of the randomized withdrawal period. The endpoint measurement was defined as the last post-randomization treatment week at which a valid ADHD-RS Total Score and CGI-S were observed. Treatment failure was defined as a ≥50% increase (worsening) in the ADHD-RS Total Score and a ≥2-point increase in the CGI-S score compared to scores at entry into the double-blind randomized withdrawal phase. Subjects who withdrew from the randomized withdrawal period and who did not provide efficacy data at their last on-treatment visit were classified as treatment failures (Study 6, Figure 5).
Adults: Short-Term Treatment in ADHD
A double-blind, randomized, placebo-controlled, parallel-group study (Study 7) was conducted in adults ages 18 to 55 (N=420) who met DSM-IV criteria for ADHD. In this study, patients were randomized to receive final doses of 30 mg, 50 mg, or 70 mg of VYVANSE or placebo for a total of four weeks of treatment. All patients receiving VYVANSE were initiated on 30 mg for the first week of treatment. Patients assigned to the 50 mg and 70 mg dose groups were titrated by 20 mg per week until they achieved their assigned dose. The primary efficacy outcome was change in Total Score from baseline to endpoint in investigator ratings on the ADHD Rating Scale (ADHD-RS). Endpoint was defined as the last post-randomization treatment week (i.e. Weeks 1 through 4) for which a valid score was obtained. All VYVANSE dose groups were superior to placebo in the primary efficacy outcome (Study 7 in Table 7).
The second study was a multi-center, randomized, double-blind, placebo-controlled, cross-over, modified analog classroom study (Study 8) of VYVANSE to simulate a workplace environment in 142 adults ages 18 to 55 who met DSM-IV-TR criteria for ADHD. There was a 4-week open-label, dose optimization phase with VYVANSE (30 mg/day, 50 mg/day, or 70 mg/day in the morning). Patients were then randomized to one of two treatment sequences: 1) VYVANSE (optimized dose) followed by placebo, each for one week, or 2) placebo followed by VYVANSE, each for one week. Efficacy assessments occurred at the end of each week, using the Permanent Product Measure of Performance (PERMP), a skill-adjusted math test that measures attention in ADHD. PERMP total score results from the sum of the number of math problems attempted plus the number of math problems answered correctly. VYVANSE treatment, compared to placebo, resulted in a statistically significant improvement in attention across all post-dose time points, as measured by average PERMP total scores over the course of one assessment day, as well as at each time point measured. The PERMP assessments were administered at pre-dose (-0.5 hours) and at 2, 4, 8, 10, 12, and 14 hours post-dose (Study 8 in Table 7, Figure 6).
Adults: Maintenance Treatment in ADHD
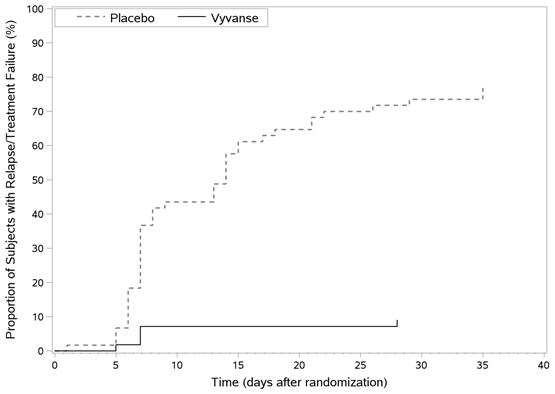
A double-blind, placebo-controlled, randomized withdrawal design study (Study 9) was conducted in adults ages 18 to 55 (N=123) who had a documented diagnosis of ADHD or met DSM-IV criteria for ADHD. At study entry, patients must have had documentation of treatment with VYVANSE for a minimum of 6 months and had to demonstrate treatment response as defined by Clinical Global Impression Severity (CGI-S) ≤3 and Total Score on the ADHD-RS <22. ADHD-RS Total Score is a measure of core symptoms of ADHD. The CGI-S score assesses the clinician's impression of the patient's current illness state and ranges from 1 (not at all ill) to 7 (extremely ill). Patients that maintained treatment response at week 3 of the open label treatment phase (N=116) were eligible to be randomized to ongoing treatment with the same dose of VYVANSE (N=56) or switched to placebo (N=60) during the double-blind phase. Patients were observed for relapse (treatment failure) during the 6-week double-blind phase. The efficacy endpoint was the proportion of patients with treatment failure during the double-blind phase. Treatment failure was defined as a ≥50% increase (worsening) in the ADHD-RS Total Score and ≥2-point increase in the CGI-S score compared to scores at entry into the double-blind phase. Maintenance of efficacy for patients treated with VYVANSE was demonstrated by the significantly lower proportion of patients with treatment failure (9%) compared to patients receiving placebo (75%) at endpoint during the double-blind phase (Study 9, Figure 7).
Table 7. Summary of Primary Efficacy Results from Short-term Studies of VYVANSE in Children, Adolescents, and Adults with ADHD:
| Study Number (Age range) | Primary Endpoint | Treatment Group | Mean Baseline Score (SD) | LS Mean Change from Baseline (SE) | Placebo-subtracted Difference* (95% CI) |
|---|---|---|---|---|---|
| Study 1 (6-12 years) | ADHD-RS-IV | VYVANSE (30 mg/day)† | 43.2 (6.7) | -21.8 (1.6) | -15.6 (-19.9, -11.2) |
| VYVANSE (50 mg/day)† | 43.3 (6.7) | -23.4 (1.6) | -17.2 (-21.5, -12.9) | ||
| VYVANSE (70 mg/day)† | 45.1(6.8) | -26.7 (1.5) | -20.5 (-24.8, -16.2) | ||
| Placebo | 42.4 (7.1) | -6.2 (1.6) | -- | ||
| Study 2 (6 - 12 years) | Average SKAMP-DS | VYVANSE (30, 50 or 70 mg/day)† | --‡ | 0.8 (0.1)§ | -0.9 (-1.1, -0.7) |
| Placebo | --‡ | 1.7 (0.1)§ | -- | ||
| Study 3 (6-12 years) | Average SKAMP-DS | VYVANSE (30, 50 or 70 mg/day)† | 0.9 (1.0)¶ | 0.7 (0.1)§ | -0.7 (-0.9, -0.6) |
| Placebo | 0.7 (0.9)¶ | 1.4 (0.1)§ | -- | ||
| Study 4 (13 - 17 years) | ADHD-RS-IV | VYVANSE (30 mg/day)† | 38.3 (6.7) | -18.3 (1.2) | -5.5 (-9.0, -2.0) |
| VYVANSE (50 mg/day)† | 37.3 (6.3) | -21.1 (1.3) | -8.3 (-11.8, -4.8) | ||
| VYVANSE (70 mg/day)† | 37.0 (7.3) | -20.7 (1.3) | -7.9 (-11.4, -4.5) | ||
| Placebo | 38.5 (7.1) | -12.8 (1.2) | -- | ||
| Study 5 (6-17 years) | ADHD-RS-IV | VYVANSE (30, 50 or 70 mg/day)† | 40.7 (7.3) | -24.3 (1.2) | -18.6 (-21.5, -15.7) |
| Placebo | 41.0 (7.1) | -5.7 (1.1) | -- | ||
| Study 7 (18-55 years) | ADHD-RS-IV | VYVANSE (30 mg/day)† | 40.5 (6.2) | -16.2 (1.1) | -8.0 (-11.5, -4.6) |
| VYVANSE (50 mg/day)† | 40.8 (7.3) | -17.4 (1.0) | -9.2 (-12.6, -5.7) | ||
| VYVANSE (70 mg/day)† | 41.0 (6.0) | -18.6 (1.0) | -10.4 (-13.9, -6.9) | ||
| Placebo | 39.4 (6.4) | -8.2 (1.4) | -- | ||
| Study 8 (18-55 years) | Average PERMP | VYVANSE (30, 50 or 70 mg/day)† | 260.1 (86.2)¶ | 312.9 (8.6)§ | 23.4 (15.6, 31.2) |
| Placebo | 261.4 (75.0)¶ | 289.5 (8.6)§ | -- |
SD: standard deviation; SE: standard error; LS Mean: least-squares mean; CI: confidence interval.
* Difference (drug minus placebo) in least-squares mean change from baseline.
† Doses statistically significantly superior to placebo.
‡ Pre-dose SKAMP-DS was not collected.
§ LS Mean for SKAMP-DS (Study 2 and 3) or PERMP (Study 8) is post-dose average score over all sessions of the treatment day, rather than change from baseline.
¶ Pre-dose SKAMP-DS (Study 3) or PERMP (Study 8) total score, averaged over both periods.
Figure 4. LS Mean SKAMP Deportment Subscale Score by Treatment and Time-point for Children Ages 6 to 12 with ADHD after 1 Week of Double Blind Treatment (Study 3):
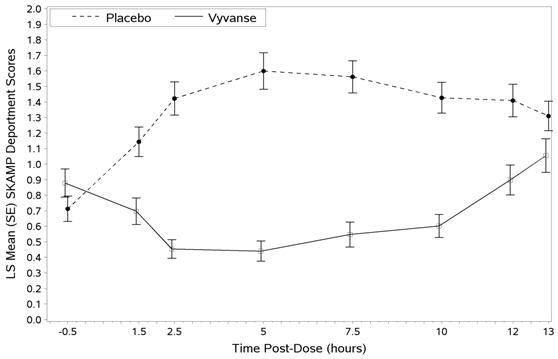
Higher score on the SKAMP-Deportment scale indicates more severe symptoms
Figure 5. Kaplan-Meier Estimated Proportion of Patients with Treatment Failure for Children and Adolescent Ages 6-17 (Study 6):
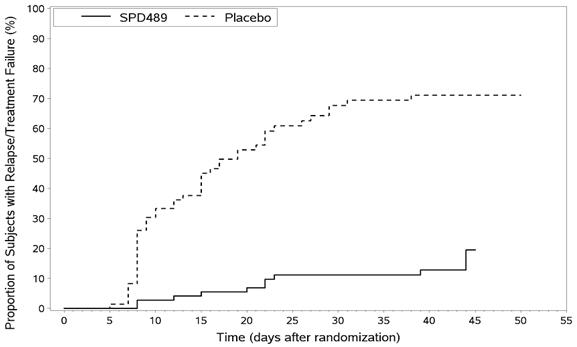
Figure 6. LS Mean (SE) PERMP Total Score by Treatment and Time-point for Adults Ages 18 to 55 with ADHD after 1 Week of Double Blind Treatment (Study 8):
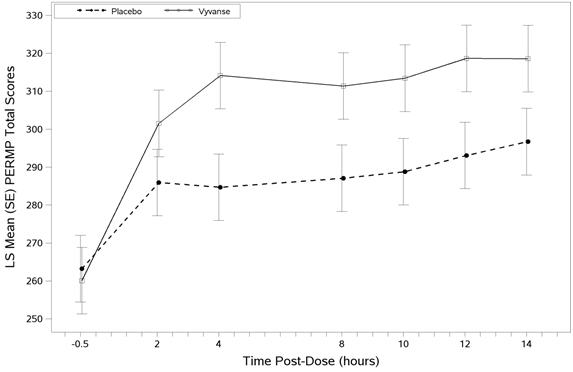
Higher score on the PERMP scale indicates less severe symptoms.
Figure 7. Kaplan-Meier Estimated Proportion of Subjects with Relapse in Adults with ADHD (Study 9):
14.2 Binge Eating Disorder (BED)
A phase 2 study evaluated the efficacy of VYVANSE 30, 50 and 70 mg/day compared to placebo in reducing the number of binge days/week in adults with at least moderate to severe BED. This randomized, double-blind, parallel-group, placebo-controlled, forced-dose titration study (Study 10) consisted of an 11-week double-blind treatment period (3 weeks of forced-dose titration followed by 8 weeks of dose maintenance). VYVANSE 30 mg/day was not statistically different from placebo on the primary endpoint. The 50 and 70 mg/day doses were statistically superior to placebo on the primary endpoint.
The efficacy of VYVANSE in the treatment of BED was demonstrated in two 12-week randomized, double-blind, multi-center, parallel-group, placebo-controlled, dose-optimization studies (Study 11 and Study 12) in adults aged 18-55 years (Study 11: N=374, Study 12: N=350) with moderate to severe BED. A diagnosis of BED was confirmed using DSM-IV criteria for BED. Severity of BED was determined based on having at least 3 binge days per week for 2 weeks prior to the baseline visit and on having a Clinical Global Impression Severity (CGI-S) score of ≥4 at the baseline visit. For both studies, a binge day was defined as a day with at least 1 binge episode, as determined from the subject's daily binge diary.
Both 12-week studies consisted of a 4-week dose-optimization period and an 8-week dose-maintenance period. During dose-optimization, subjects assigned to VYVANSE began treatment at the titration dose of 30 mg/day and, after 1 week of treatment, were subsequently titrated to 50mg/day. Additional increases to 70 mg/day were made as tolerated and clinically indicated. Following the dose-optimization period, subjects continued on their optimized dose for the duration of the dose-maintenance period.
The primary efficacy outcome for the two studies was defined as the change from baseline at Week 12 in the number of binge days per week. Baseline is defined as the weekly average of the number of binge days per week for the 14 days prior to the baseline visit. Subjects from both studies on VYVANSE had a statistically significantly greater reduction from baseline in mean number of binge days per week at Week 12. In addition, subjects on VYVANSE showed greater improvement as compared to placebo across key secondary outcomes with higher proportion of subjects rated improved on the CGI-I rating scale, higher proportion of subjects with 4-week binge cessation, and greater reduction in the Yale-Brown Obsessive Compulsive Scale Modified for Binge Eating (Y-BOCS-BE) total score.
Table 8. Summary of Primary Efficacy Results in BED:
| Study Number | Treatment Group | Primary Efficacy Measure: Binge Days per Week at Week 12 | ||
|---|---|---|---|---|
| Mean Baseline Score (SD) | LS Mean Change from Baseline (SE) | Placebo-subtracted Difference* (95% CI) | ||
| Study 11 | VYVANSE (50 or 70 mg/day)† | 4.79 (1.27) | -3.87 (0.12) | -1.35 (-1.70, -1.01) |
| Placebo | 4.60 (1.21) | -2.51 (0.13) | -- | |
| Study 12 | VYVANSE (50 or 70 mg/day)† | 4.66 (1.27) | -3.92 (0.14) | -1.66 (-2.04, -1.28) |
| Placebo | 4.82 (1.42) | -2.26 (0.14) | -- | |
SD: standard deviation; SE: standard error; LS Mean: least-squares mean; CI: confidence interval.
*
†
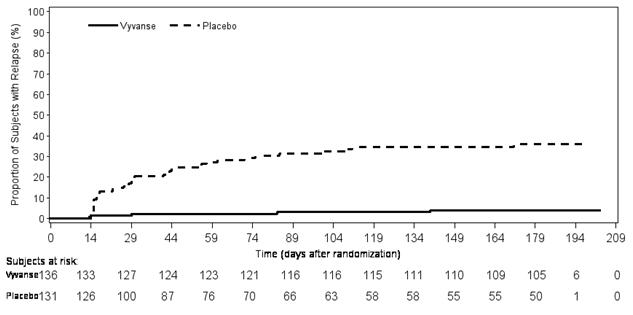
A double-blind, placebo controlled, randomized withdrawal design study (Study 13) was conducted to evaluate maintenance of efficacy based on time to relapse between VYVANSE and placebo in adults aged 18 to 55 (N=267) with moderate to severe BED. In this longer-term study patients who had responded to VYVANSE in the preceding 12-week open-label treatment phase were randomized to continuation of VYVANSE or placebo for up to 26 weeks of observation for relapse. Response in the open-label phase was defined as 1 or fewer binge days each week for four consecutive weeks prior to the last visit at the end of the 12-week open-label phase and a CGI-S score of 2 or less at the same visit. Relapse during the double-blind phase was defined as having 2 or more binge days each week for two consecutive weeks (14 days) prior to any visit and having an increase in CGI-S score of 2 or more points compared to the randomized-withdrawal baseline. Maintenance of efficacy for patients who had an initial response during the open-label period and then continued on VYVANSE during the 26-week double-blind randomized-withdrawal phase was demonstrated with VYVANSE being superior over placebo as measured by time to relapse.
Figure 8. Kaplan-Meier Estimated Proportion of Subjects with Relapse in Adults with BED (Study 13):
Examination of population subgroups based on age (there were no patients over 65), gender, and race did not reveal any clear evidence of differential responsiveness in the treatment of BED.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.