XULANE Patch Ref.[10487] Active ingredients: 17 alpha-Ethinylestradiol Norelgestromin
Source: FDA, National Drug Code (US) Revision Year: 2020
4. Contraindications
Xulane is contraindicated in women with the following conditions:
- At high risk of arterial or venous thromboembolic events. Examples include women who:
- Smoke, if over age 35 [see Boxed Warning, and Warnings and Precautions (5.1)]
- Have deep vein thrombosis or pulmonary embolism, now or in the past [see Warnings and Precautions (5.1)]
- Have inherited or acquired hypercoagulopathies [see Warnings and Precautions (5.1)]
- Have cerebrovascular disease [see Warnings and Precautions (5.1)]
- Have coronary artery disease [see Warnings and Precautions (5.1)]
- Have thrombogenic valvular or thrombogenic rhythm diseases of the heart (for example, subacute bacterial endocarditis with valvular disease, or atrial fibrillation) [see Warnings and Precautions (5.1)]
- Have uncontrolled hypertension [see Warnings and Precautions (5.5)]
- Have diabetes mellitus with vascular disease [see Warnings and Precautions (5.7)]
- Have headaches with focal neurological symptoms or have migraine headaches with aura
- Women over age 35 with any migraine headaches [see Warnings and Precautions (5.8)]
- Body Mass Index ≥30 kg/m2 [see Warnings and Precautions (5.1)]
- Liver tumors, benign or malignant, or liver disease [see Warnings and Precautions (5.3), Use in Specific Populations (8.6) and Clinical Pharmacology (12.3)]
- Undiagnosed abnormal uterine bleeding [see Warnings and Precautions (5.9)]
- Pregnancy, because there is no reason to use hormonal contraceptives during pregnancy [see Warnings and Precautions (5.10) and Use in Specific Populations (8.1)]
- Breast cancer or other estrogen- or progestin-sensitive cancer, now or in the past [see Warnings and Precautions (5.12)]
- Use of Hepatitis C drug combinations containing ombitasvir/paritaprevir/ritonavir, with or without dasabuvir, due to the potential for alanine aminotransferase (ALT) elevations [see Warnings and Precautions (5.4)]
5. Warnings and Precautions
5.1 Thromboembolic Disorders and Other Vascular Conditions
- Stop Xulane if an arterial or venous thromboembolic event (VTE) occurs.
- Stop Xulane if there is unexplained loss of vision, proptosis, diplopia, papilledema, or retinal vascular lesions. Evaluate for retinal vein thrombosis immediately.
- If feasible, stop Xulane at least 4 weeks before and through 2 weeks after major surgery or other surgeries known to have an elevated risk of VTE. Discontinue use of Xulane during prolonged immobilization and resume treatment based on clinical judgment.
- Start Xulane no earlier than 4 weeks after delivery, in women who are not breastfeeding. The risk of postpartum VTE decreases after the third postpartum week, whereas the risk of ovulation increases after the third postpartum week.
- Before starting Xulane, evaluate any past medical history or family history of thrombotic or thromboembolic disorders and consider whether the history suggests an inherited or acquired hypercoagulopathy. [see Contraindications (4)].
Arterial Events
The use of CHCs increases the risk of cardiovascular events and cerebrovascular events, such as myocardial infarction and stroke. The risk is greater among older women (>35 years of age), smokers, and women with hypertension, dyslipidemia, diabetes, or obesity. Xulane is contraindicated in women over 35 years of age who smoke [see Contraindications (4)]. Cigarette smoking increases the risk of serious cardiovascular events from CHC use. This risk increases with age, particularly in women over 35 years of age, and with the number of cigarettes smoked.
Venous Events
The use of CHCs increases the risk of venous thromboembolic events (VTEs), such as deep vein thrombosis and pulmonary embolism. Risk factors for VTEs include smoking, obesity, and family history of VTE, in addition to other factors that contraindicate use of CHCs. The risk of VTE may be greater with Xulane in women with a BMI ≥30 kg/m2 compared to women with a lower BMI [see Contraindications (4)].
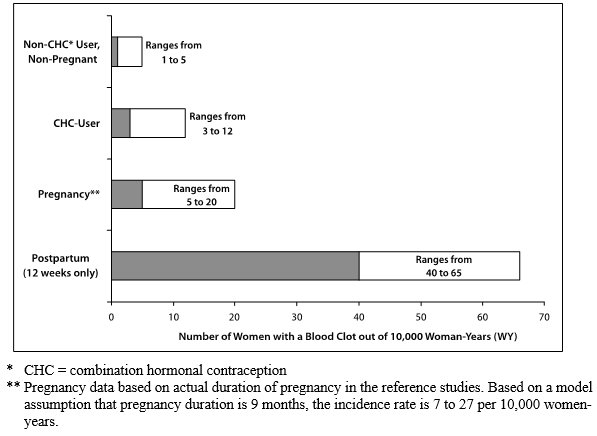
While the increased risk of VTE associated with use of CHCs is well-established, the rates of VTE are even greater during pregnancy, and especially during the postpartum period (see Figure 1). The frequency of VTE in women using CHCs has been estimated to be 3 to 12 cases per 10,000 woman-years.
The risk of VTE is highest during the first year of use of CHCs and when restarting hormonal contraception after a break of 4 weeks or longer. This initial higher risk declines during the first year, but users of CHCs remain at an increased risk of VTE compared to non-users of CHCs. Based on results from a few studies, there is some evidence that this is true for non-oral products as well. The risk of thromboembolic disease due to CHCs gradually disappears after CHC use is discontinued.
Figure 1 shows the risk of developing a VTE for women who are not pregnant and do not use CHCs, for women who use CHCs with a range of doses and routes of administration, for pregnant women, and for women in the postpartum period. To put the risk of developing a VTE into perspective: If 10,000 women who are not pregnant and do not use CHCs are followed for one year, between 1 and 5 of these women will develop a VTE.
Figure 1. Likelihood of Developing a VTE Within One Year Among Preg nant and Non-Preg nant Women:
5.2 Ethinyl Estradiol Exposure
Higher estrogen exposure may increase the risk of adverse reactions, including venous thromboembolism (VTE). The Area Under the Curve (AUC) for ethinyl estradiol (EE) is approximately 60% higher in women using XULANE compared to oral contraceptives containing EE 35 mcg. In contrast, the peak concentration (Cmax) for EE is approximately 25% lower in women using norelgestromin and ethinyl estradiol transdermal system [see Clinical Pharmacology (12.3)].
5.3 Liver Disease
Impaired Liver Function
Do not use Xulane in women with liver disease, such as acute viral hepatitis or severe (decompensated) cirrhosis of liver [see Contraindications (4)]. Discontinue Xulane if jaundice develops. Acute or chronic disturbances of liver function may necessitate the discontinuation of CHC use until markers of liver function return to normal and CHC causation has been excluded.
Liver Tumors
Xulane is contraindicated in women with benign and malignant liver tumors [see Contraindications (4)]. Hepatic adenomas are associated with CHC use. An estimate of the attributable risk is 3.3 cases/100,000 CHC users. Rupture of hepatic adenomas may cause death through intra-abdominal hemorrhage.
Studies have shown an increased risk of developing hepatocellular carcinoma in long-term (>8 years) CHC users. However, the risk of liver cancers in CHC users is less than one case per million users.
5.4 Risk of Liver Enzyme Elevations with Concomitant Hepatitis C Treatment
During clinical trials with the Hepatitis C combination drug regimen that contains ombitasvir/paritaprevir/ritonavir, with or without dasabuvir, ALT elevations greater than 5 times the upper limit of normal (ULN), including some cases greater than 20 times the ULN, were significantly more frequent in women using ethinyl estradiol-containing medications, such as CHCs. Discontinue Xulane prior to starting therapy with the combination drug regimen ombitasvir/paritaprevir/ritonavir, with or without dasabuvir [see Contraindications (4)]. Xulane can be restarted approximately 2 weeks following completion of treatment with the Hepatitis C combination drug regimen.
5.5 High Blood Pressure
Xulane is contraindicated in women with uncontrolled hypertension or hypertension with vascular disease [see Contraindications (4)]. For women with well-controlled hypertension, monitor blood pressure and stop Xulane if blood pressure rises significantly.
An increase in blood pressure has been reported in women taking hormonal contraceptives, and this increase is more likely in older women with extended duration of use. The incidence of hypertension increases with increasing concentrations of progestin.
5.6 Gallbladder Disease
Studies suggest a small increased relative risk of developing gallbladder disease among CHC users. Use of CHCs may also worsen existing gallbladder disease. A past history of CHC-related cholestasis predicts an increased risk with subsequent CHC use. Women with a history of pregnancy-related cholestasis may be at an increased risk for CHC-related cholestasis.
5.7 Carbohydrate and Lipid Metabolic Effects
Carefully monitor prediabetic and diabetic women who take Xulane. CHCs may decrease glucose tolerance in a dose-related fashion. In a 6-cycle clinical trial with norelgestromin and ethinyl estradiol transdermal system there were no clinically significant changes in fasting blood glucose from baseline to end of treatment.
Consider alternative contraception for women with uncontrolled dyslipidemia. A small proportion of women will have adverse lipid changes while on hormonal contraceptives.
Women with hypertriglyceridemia, or a family history thereof, may be at an increased risk of pancreatitis when using hormonal contraceptives.
5.8 Headache
If a woman taking Xulane develops new headaches that are recurrent, persistent or severe, evaluate the cause and discontinue Xulane if indicated.
Consider discontinuation of Xulane in the case of increased frequency or severity of migraine during hormonal contraceptive use (which may be prodromal of a cerebrovascular event).
5.9 Bleeding Irregularities
Unscheduled Bleeding and Spotting
Unscheduled (breakthrough) bleeding and spotting sometimes occur in women using norelgestromin and ethinyl estradiol transdermal system. Consider non-hormonal causes and take adequate diagnostic measures to rule out malignancy, other pathology, or pregnancy in the event of unscheduled bleeding, as in the case of any abnormal vaginal bleeding. If pathology and pregnancy have been excluded, time or a change to another contraceptive product may resolve the bleeding.
In the clinical trials, most women started their scheduled (withdrawal) bleeding on the fourth day of the drug-free interval, and the median duration of withdrawal bleeding was 5 to 6 days. On average, 26% of women per cycle had 7 or more total days of bleeding and/or spotting (this includes both scheduled and unscheduled bleeding and/or spotting). Three clinical studies of the efficacy of norelgestromin and ethinyl estradiol transdermal system in preventing pregnancy assessed scheduled and unscheduled bleeding [see Clinical Studies (14)] in 3,330 women who completed 22,155 cycles of exposure. A total of 36 (1.1%) of the women discontinued norelgestromin and ethinyl estradiol transdermal system at least in part, due to bleeding or spotting.
Table 1 summarizes the proportion of subjects who experienced unscheduled (breakthrough) bleeding/spotting by treatment cycle.
Table 1. Unscheduled (Breakthrough) Bleeding/Spotting (Subjects Evaluable for Efficacy):
| Treatment Cycle | Pooled data from 3 studies | |
|---|---|---|
| N=3319 | ||
| n | %* | |
| Cycle 1 | 2994 | 18.2 |
| Cycle 2 | 2743 | 11.9 |
| Cycle 3 | 2699 | 11.6 |
| Cycle 4 | 2541 | 10.1 |
| Cycle 5 | 2532 | 9.2 |
| Cycle 6 | 2494 | 8.3 |
| Cycle 7 | 698 | 8.3 |
| Cycle 8 | 692 | 8.7 |
| Cycle 9 | 654 | 8.6 |
| Cycle 10 | 621 | 8.7 |
| Cycle 11 | 631 | 8.9 |
| Cycle 12 | 617 | 6.3 |
| Cycle 13 | 611 | 8.0 |
* Percentage of subjects with breakthrough bleeding/spotting events.
Amenorrhea and Oligomenorrhea
In the event of amenorrhea, consider the possibility of pregnancy. If the patient has not adhered to the prescribed dosing schedule (missed one patch or started the patch on a day later than she should have), consider the possibility of pregnancy at the time of the first missed period and take appropriate diagnostic measures. If the patient has adhered to the prescribed regimen and misses two consecutive periods, rule out pregnancy.
Some women may encounter amenorrhea or oligomenorrhea after discontinuation of hormonal contraceptive use, especially when such a condition was pre-existent.
5.10 Hormonal Contraceptive Use Before or During Early Pregnancy
Extensive epidemiological studies have revealed no increased risk of birth defects in women who have used oral contraceptives prior to pregnancy. Studies also do not suggest a teratogenic effect, particularly in so far as cardiac anomalies and limb reduction defects are concerned, when oral contraceptives are taken inadvertently during early pregnancy. Discontinue Xulane use if pregnancy is confirmed.
Administration of CHCs should not be used as a test for pregnancy [see Use in Specific Populations (8.1)].
5.11 Depression
Carefully observe women with a history of depression and discontinue Xulane if depression recurs to a serious degree.
5.12 Carcinoma of Breasts and Cervix
Xulane is contraindicated in women who currently have or have had breast cancer because breast cancer may be hormonally sensitive [see Contraindications (4)].
There is substantial evidence that CHCs do not increase the incidence of breast cancer. Although some past studies have suggested that CHCs might increase the incidence of breast cancer, more recent studies have not confirmed such findings.
Some studies suggest that combination oral contraceptive use has been associated with an increase in the risk of cervical cancer or intraepithelial neoplasia. However, there continues to be controversy about the extent to which such findings may be due to differences in sexual behavior and other factors.
5.13 Effect on Binding Globulins
The estrogen component of CHCs may raise the serum concentrations of thyroxine-binding globulin, sex hormone-binding globulin and cortisol-binding globulin. The dose of replacement thyroid hormone or cortisol therapy may need to be increased.
5.14 Monitoring
A woman who is taking hormonal contraceptive should have a yearly visit with her healthcare provider for a blood pressure check and for other indicated healthcare.
5.15 Hereditary Angioedema
In women with hereditary angioedema, exogenous estrogens may induce or exacerbate symptoms of angioedema.
5.16 Chloasma
Chloasma may occasionally occur, especially in women with a history of chloasma gravidarum. Women with a tendency to chloasma should avoid exposure to the sun or ultraviolet radiation while using Xulane.
6. Adverse Reactions
The following serious adverse reactions with the use of combination hormonal contraceptives, including Xulane, are discussed elsewhere in the labeling:
- Serious cardiovascular events and stroke [see Boxed Warning and Warnings and Precautions (5.1)]
- Vascular events, including venous and arterial thromboembolic events [see Warnings and Precautions (5.1)]
- Liver disease [see Warnings and Precautions (5.3)]
Adverse reactions commonly reported by users of combination hormonal contraceptives are:
- Irregular uterine bleeding
- Nausea
- Breast tenderness
- Headache
6.1. Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
The data described below reflect exposure to norelgestromin and ethinyl estradiol transdermal system in 3330 sexually active women (3322 of whom had safety data) who participated in three Phase 3 clinical trials designed to evaluate contraceptive efficacy and safety. These subjects received six or 13 cycles of contraception (norelgestromin and ethinyl estradiol transdermal system or an oral contraceptive comparator in 2 of the trials). The women ranged in age from 18 to 45 years and were predominantly white (91%).
The most common adverse reactions (≥5%) reported during clinical trials were breast symptoms, nausea/vomiting, headache, application site disorder, abdominal pain, dysmenorrhea, vaginal bleeding and menstrual disorders, and mood, affect and anxiety disorders. The most common events leading to discontinuation were application site reaction, breast symptoms (including breast discomfort, engorgement and pain), nausea and/or vomiting, headache and emotional lability.
Adverse drug reactions reported by ≥2.5% of norelgestromin and ethinyl estradiol transdermal system-treated subjects in these trials are shown in Table 2.
Table 2. Adverse Drug Reactions Reported by ≥2.5% of Norelgestromin and Ethinyl Estradiol Transdermal System-treated Subjects in Three Phase 3 Clinical Trials:
| System/Organ Class* Adverse reaction | Norelgestromin and Ethinyl Estradiol Transdermal System (n=3322) |
|---|---|
| Reproductive system and breast disorders | |
| Breast symptoms† | 22.4% |
| Dysmenorrhea | 7.8% |
| Vaginal bleeding and menstrual disorders† | 6.4% |
| Gastrointestinal disorders | |
| Nausea | 16.6% |
| Abdominal pain† | 8.1% |
| Vomiting | 5.1% |
| Diarrhea | 4.2% |
| Nervous system disorders | |
| Headache | 21.0% |
| Dizziness | 3.3% |
| Migraine | 2.7% |
| General disorders and administration site conditions | |
| Application site disorder† | 17.1% |
| Fatigue | 2.6% |
| Psychiatric disorders | |
| Mood, affect and anxiety disorders† | 6.3% |
| Skin and subcutaneous tissue disorders | |
| Acne | 2.9% |
| Pruritus | 2.5% |
| Infections and infestations | |
| Vaginal yeast infection† | 3.9% |
| Investigations | |
| Weight increased | 2.7% |
* MedDRA version 10.0
† Represents a bundle of similar terms
Additional adverse drug reactions that occurred in <2.5% of norelgestromin and ethinyl estradiol transdermal system-treated subjects in the above clinical trials datasets are:
- Gastrointestinal disorders: Abdominal distension
- General disorders and administration site conditions: Fluid retention1, malaise
- Hepatobiliary disorders: Cholecystitis
- Investigations: Blood pressure increased, lipid disorders1
- Musculoskeletal and connective tissue disorders: Muscle spasms
- Psychiatric disorders: Insomnia, libido decreased, libido increased
- Reproductive system and breast disorders: Galactorrhea, genital discharge, premenstrual syndrome, uterine spasm, vaginal discharge, vulvovaginal dryness
- Respiratory, thoracic and mediastinal disorders: Pulmonary embolism
- Skin and subcutaneous tissue disorders: Chloasma, dermatitis contact, erythema, skin irritation
1 Represents a bundle of similar terms
6.2. Postmarketing Experience
The following adverse reactions (Table 3) have been identified during postapproval use of norelgestromin and ethinyl estradiol transdermal system. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Table 3. Alphabetical List of Adverse Drug Reactions Identified During Postmarketing Experience with Norelgestromin and Ethinyl Estradiol Transdermal System by System Organ Class*:
| System Organ Class | Adverse Drug Reactions |
|---|---|
| Cardiac disorders | Myocardial infarction† |
| Endocrine disorders | Hyperglycemia, insulin resistance |
| Eye disorders | Contact lens intolerance or complication |
| Gastrointestinal disorders | Colitis |
| General disorders and administration site conditions | Application site reaction†, edema† |
| Hepatobiliary disorders | Blood cholesterol abnormal, cholelithiasis, cholestasis, hepatic lesion, jaundice cholestatic, low density lipoprotein increased |
| Immune system disorders | Allergic reaction†, urticaria |
| Investigations | Blood glucose abnormal, blood glucose decreased |
| Metabolism and nutrition disorders | Increased appetite |
| Neoplasms benign, malignant and unspecified (Incl. cysts and polyps) | Breast cancer†, cervix carcinoma, hepatic adenoma, hepatic neoplasm |
| Nervous system disorders | Dysgeusia, migraine with aura |
| Psychiatric disorders | Anger, emotional disorder, frustration, irritability |
| Reproductive system and breast disorders | Breast mass, cervical dysplasia, fibroadenoma of breast, menstrual disorder†, suppressed lactation, uterine leiomyoma |
| Skin and subcutaneous tissues disorders | Alopecia, eczema, erythema multiforme, erythema nodosum, photosensitivity reaction, pruritus generalized, rash†, seborrheic dermatitis, skin reaction |
| Vascular disorders | Arterial thrombosis†, cerebrovascular accident†, deep vein thrombosis†, hemorrhage intracranial†, hypertension, hypertensive crisis, pulmonary embolism†, thrombosis† |
* MedDRA version 10.0
† Represents a bundle of similar terms
7. Drug Interactions
Consult the labeling of concurrently-used drugs to obtain further information about interactions with hormonal contraceptives or the potential for enzyme alterations.
7.1 Effects of Other Drugs on Combined Hormonal Contraceptives
Substances Decreasing the Plasma Concentrations of CHCs and Potentially Diminishing the Efficacy of CHCs
Drugs or herbal products that induce certain enzymes, including cytochrome P450 3A4 (CYP3A4), may decrease the plasma concentrations of CHCs and potentially diminish the effectiveness of CHCs or increase breakthrough bleeding. Some drugs or herbal products that may decrease the effectiveness of hormonal contraceptives include phenytoin, barbiturates, carbamazepine, bosentan, felbamate, griseofulvin, oxcarbazepine, rifampicin, topiramate, rifabutin, rufinamide, aprepitant, and products containing St. John's wort. Interactions between hormonal contraceptives and other drugs may lead to breakthrough bleeding and/or contraceptive failure. Counsel women to use an alternative method of contraception or a back-up method when enzyme inducers are used with CHCs, and to continue back-up contraception for 28 days after discontinuing the enzyme inducer to ensure contraceptive reliability.
Substances Increasing the Plasma Concentrations of CHCs
Co-administration of atorvastatin or rosuvastatin and certain CHCs containing EE increase AUC values for EE by approximately 20% to 25%. Ascorbic acid and acetaminophen may increase plasma EE concentrations, possibly by inhibition of conjugation. CYP3A4 inhibitors such as itraconazole, voriconazole, fluconazole, grapefruit juice, or ketoconazole may increase plasma hormone concentrations.
Human Immunodeficiency Virus (HIV)/Hepatitis C Virus (HCV) Protease Inhibitors and Non-Nucleoside Reverse Transcriptase Inhibitors
Significant changes (increase or decrease) in the plasma concentrations of estrogen and/or progestin have been noted in some cases of co-administration with HIV protease inhibitors (decrease [e.g., nelfinavir, ritonavir, darunavir/ritonavir, (fos)amprenavir/ritonavir, lopinavir/ritnoavir, and tipranavir/ritonavir] or increase [e.g., indinavir and atazanavir/ritonavir])/HCV protease inhibitors or with non-nucleoside reverse transcriptase inhibitors (decrease [e.g., nevirapine] or increase [e.g., etravirine]).
7.2 Effects of Combined Hormonal Contraceptives on Other Drugs
CHCs containing EE may inhibit the metabolism of other compounds (e.g., cyclosporine, prednisolone, theophylline, tizanidine, and voriconazole) and increase their plasma concentrations. CHCs have been shown to decrease plasma concentrations of acetaminophen, clofibric acid, morphine, salicylic acid, and temazepam. Significant decrease in plasma concentration of lamotrigine has been shown, likely due to induction of lamotrigine glucuronidation. This may reduce seizure control; therefore, dosage adjustments of lamotrigine may be necessary.
Women on thyroid hormone replacement therapy may need increased doses of thyroid hormone because serum concentration of thyroid-binding globulin increases with use of CHCs [see Warnings and Precautions (5.13)].
7.3 Concomitant Use with HCV Combination Therapy – Liver Enzyme Elevation
Do not co-administer Xulane with HCV drug combinations containing ombitasvir/paritaprevir/ritonavir, with or without dasabuvir, due to potential for ALT elevations [see Warnings and Precautions (5.4)].
7.4 Interference with Laboratory Tests
The use of contraceptive steroids may influence the results of certain laboratory tests, such as coagulation factors, lipids, glucose tolerance, and binding proteins.
8.1. Pregnancy
There is little or no increased risk of birth defects in women who inadvertently use hormonal contraceptives during early pregnancy. Epidemiologic studies and meta-analyses have not found an increased risk of genital or non-genital birth defects (including cardiac anomalies and limb reduction defects) following exposure to low dose hormonal contraceptives prior to conception or during early pregnancy.
The administration of hormonal contraceptives to induce withdrawal bleeding should not be used as a test for pregnancy. Hormonal contraceptives should not be used during pregnancy to treat threatened or habitual abortion.
8.3. Nursing Mothers
The effects of Xulane in nursing mothers have not been evaluated and are unknown. When possible, advise the nursing mother to use other forms of contraception until she has completely weaned her child. Estrogen-containing CHCs can reduce milk production in breastfeeding mothers. This is less likely to occur once breastfeeding is well-established; however, it can occur at any time in some women. Small amounts of contraceptive steroids and/or metabolites are present in breast milk.
8.4. Pediatric Use
Safety and efficacy of norelgestromin and ethinyl estradiol transdermal system have been established in women of reproductive age. Efficacy is expected to be the same for post-pubertal adolescents under the age of 18 and for users 18 years and older. Use of this product before menarche is not indicated.
8.5. Geriatric Use
Xulane has not been studied in postmenopausal women and is not indicated in this population.
8.7. Renal Impairment
No studies with Xulane have been conducted in women with renal impairment.
8.6. Hepatic Impairment
No studies with Xulane have been conducted in women with hepatic impairment. However, steroid hormones may be poorly metabolized in patients with impaired liver function. Acute or chronic disturbances of liver function may necessitate the discontinuation of combined hormonal contraceptive use until markers of liver function return to normal and combined hormonal contraceptive causation has been excluded [See Contraindications (4) and Warnings and Precautions (5.3)].
8. Use in Specific Populations
8.8 BMI and Weight Considerations
Xulane is contraindicated in women with a BMI ≥30 kg/m2 because of the potential increased risk of VTE [see Contraindications (4) and Warnings and Precautions (5.1)].
Xulane may be less effective in preventing pregnancy in women who weigh 198 lbs. or more [see Clinical Studies (14)].
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.