ZALTRAP Concentrate for solution for infusion Ref.[7452] Active ingredients: Aflibercept
Source: European Medicines Agency (EU) Revision Year: 2024 Publisher: Sanofi Winthrop Industrie, 82 avenue Raspail, 94250 Gentilly, France
Pharmacodynamic properties
Pharmacotherapeutic group: Antineoplastic agents, other antineoplastic agents
ATC code: L01XX44
Mechanism of action
Vascular endothelial growth factor A and B (VEGF-A, VEGF-B), and placental growth factor (PlGF) are members of the VEGF family of angiogenic factors that can act as potent mitogenic, chemotactic, and vascular permeability factors for endothelial cells. VEGF-A acts via two receptor tyrosine kinases, VEGFR-1 and VEGFR-2, present on the surface of endothelial cells. PlGF and VEGF-B bind only to VEGFR-1, which is also present on the surface of leucocytes. Excessive activation of these receptors by VEGF-A can result in pathological neovascularisation and excessive vascular permeability. PlGF is also linked to pathological neovascularisation and recruitment of inflammatory cells into tumours.
Aflibercept, also known as VEGF TRAP in the scientific literature, is a recombinant fusion protein consisting of VEGF-binding portions from the extracellular domains of human VEGF receptors 1 and 2 fused to the Fc portion of the human IgG1. Aflibercept is produced by recombinant DNA technology in a Chinese hamster ovary (CHO) K-1 mammalian expression system. Aflibercept is a dimeric glycoprotein with a protein molecular weight of 97 kilodaltons (kDa) and contains glycosylation, constituting an additional 15% of the total molecular mass, resulting in a total molecular weight of 115 kDa.
Aflibercept acts as a soluble decoy receptor that binds to VEGF-A, with higher affinity than its native receptors, as well as the related ligands PlGF and VEGF-B. By acting as a ligand trap, aflibercept prevents binding of endogenous ligands to their cognate receptors and thereby blocks receptor mediated signaling.
Aflibercept blocks the activation of VEGF receptors and the proliferation of endothelial cells, thereby inhibiting the growth of new vessels that supply tumours with oxygen and nutrients.
Aflibercept binds to human VEGF-A (equilibrium dissociation constant KD of 0.5 pM for VEGF-A 165 and 0.36 pM for VEGF-A121), to human PlGF (KD of 39 pM for PlGF-2), and to human VEGF-B (KD of 1.92 pM) to form a stable, inert complex which has no detectable biological activity.
Pharmacodynamic effects
Administration of aflibercept to mice bearing xenotransplant or allotransplant tumours inhibited the growth of various cancer types.
Clinical efficacy and safety
The efficacy and safety of ZALTRAP were evaluated in a randomised, double-blind, placebo-controlled study in patients with metastatic colorectal cancer who had previously been treated with an oxaliplatin-based treatment with or without prior bevacizumab. A total of 1,226 patients were randomised (1:1) to receive either ZALTRAP (N=612; 4 mg/kg as a 1 hour intravenous infusion on day 1) or placebo (N=614), in combination with 5-fluouracil plus irinotecan [FOLFIRI: irinotecan 180 mg/m 2 intravenous infusion over 90 minutes and folinic acid (dl racemic) 400 mg/m² intravenous infusion over 2 hours at the same time on day 1 using a Y-line, followed by 5-FU 400 mg/m² intravenous bolus, followed by 5-FU 2,400 mg/m² continuous intravenous infusion over 46-hours]. The treatment cycles on both arms were repeated every 2 weeks. Patients were treated until disease progression or unacceptable toxicity. The primary efficacy endpoint was overall survival. Treatment assignment was stratified by the ECOG performance status (0 versus 1 versus 2) and according to prior therapy with bevacizumab (yes or no).
Demographics were well balanced between the treatment arms (age, race, ECOG performance status, and prior bevacizumab status). Of the 1,226 patients randomised in the study, the median age was 61 years, 58.6% were male, 97.8% had a baseline ECOG performance status (PS) of 0 or 1, and 2.2% had a baseline ECOG performance status (PS) of 2. Among the 1,226 randomised patients, 89.4% and 90.2% of patients treated with the placebo/FOLFIRI and ZALTRAP/FOLFIRI regimens, respectively, received prior oxaliplatin-based combination chemotherapy in the metastatic/advanced setting. Approximately 10% of patients (10.4% and 9.8% of patients treated with the placebo/FOLFIRI and ZALTRAP/FOLFIRI regimens, respectively) received prior oxaliplatin-based adjuvant chemotherapy and progressed on or within 6 months of completion of adjuvant chemotherapy. Oxaliplatin-based regimens were administered in combination with bevacizumab in 373 patients (30.4%).
Overall efficacy results for the ZALTRAP/FOLFIRI regimen versus the placebo/FOLFIRI regimen are summarised in Figure 1 and Table 2.
Figure 1. Overall survival (months) – Kaplan-Meier curves by treatment group – ITT population:
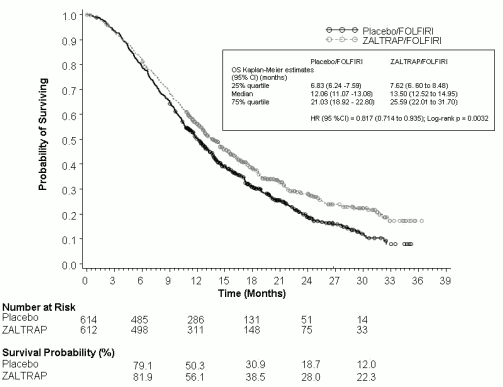
Table 2. Main efficacy endpointsa – ITT population:
| Placebo/FOLFIRI (N=614) | ZALTRAP/FOLFIRI (N=612) | |
|---|---|---|
| OS | ||
| Number of death events, n (%) | 460 (74.9%) | 403 (65.8%) |
| Median overall survival (95% CI) (months) | 12.06 (11.07 to 13.08) | 13.50 (12.52 to 14.95) |
| Stratified hazard ratio (95% CI) | 0.817 (0.714 to 0.935) | |
| Stratified log-rank test p-value | 0.0032 | |
| PFSb | ||
| Number of events, n (%) | 454 (73.9%) | 393 (64.2%) |
| Median PFS (95% CI) (months) | 4.67 (4.21 to 5.36) | 6.90 (6.51 to 7.20) |
| Stratified hazard ratio (95% CI) | 0.758 (0.661 to 0.869) | |
| Stratified log-rank test p-value | 0.00007 | |
| Overall Response Rate (CR+PR) (95% CI) (%)c | 11.1 (8.5 to 13.8) | 19.8 (16.4 to 23.2) |
| Stratified Cochran-Mantel-Haenszel test p-value | 0.0001 | |
a Stratified on ECOG performance status (0 versus 1 versus 2) and prior bevacizumab (yes versus no).
b PFS (based on tumour assessment by the IRC): Significance threshold is set to 0.0001
c Overall objective response rate by IRC
OS and PFS by stratification factors were performed. A numerically lower treatment effect on OS with the ZALTRAP/FOLFIRI regimen was reported for patients with prior bevacizumab as compared to patients without prior bevacizumab exposure, with no evidence of heterogeneity in treatment effect (non significant interaction test). Results by prior bevacizumab exposure are summarised in Table 3.
Table 3. OS and PFS by prior bevacizumab exposurea – ITT population:
| Placebo/FOLFIRI (N=614) | ZALTRAP/FOLFIRI (N=612) | |
|---|---|---|
| OS | ||
| Patients with prior bevacizumab (n (%)) | 187 (30.5%) | 186 (30.4%) |
| Median OS (95% CI) (months) | 11.7 (9.96 to 13.77) | 12.5 (10.78 to 15.47) |
| Hazard ratio (95% CI) | 0.862 (0.676 to 1.100) | |
| Patients with no prior bevacizumab (n (%)) | 427 (69.5%) | 426 (69.6%) |
| Median OS (95% CI) (months) | 12.4 (11.17 to 13.54) | 13.9 (12.72 to 15.64) |
| Hazard ratio (95% CI) | 0.788 (0.671 to 0.925) | |
| PFS | ||
| Patients with prior bevacizumab (n (%)) | 187 (30.5%) | 186 (30.4%) |
| Median PFS (95% CI) (months) | 3.9 (3.02 to 4.30) | 6.7 (5.75 to 8.21) |
| Hazard ratio (95% CI) | 0.661 (0.512 to 0.852) | |
| Patients with no prior bevacizumab (n (%)) | 427 (69.5%) | 426 (69.6%) |
| Median PFS (95% CI) (months) | 5.4 (4.53 to 5.68) | 6.9 (6.37 to 7.20) |
| Hazard ratio (95% CI) | 0.797 (0.679 to 0.936) | |
a As determined per IVRS
Analysis for OS and PFS by ECOG PS was also performed. The hazard ratio (95% CI) of overall survival was 0.77 (0.64 to 0.93) for ECOG performance status 0 and 0.87 (0.71 to 1.06) for ECOG performance status 1. The hazard ratio (95% CI) of progression free survival was 0.76 (0.63 to 0.91) for ECOG performance status 0 and 0.75 (0.61 to 0.92) for ECOG performance status 1.
Post-hoc analyses excluding patients who progressed during or within 6 months of adjuvant therapy for patients with or without prior bevacizumab treatment are summarised in Table 4.
Table 4. Post-hoc analyses excluding adjuvant patientsa,b:
| Placebo/FOLFIRI (N=550) | ZALTRAP/FOLFIRI (N=552) | |
|---|---|---|
| Patients with prior bevacizumab excluding adjuvant only (n (%)) | 179 (32.5%) | 177 (32.1%) |
| Median OS (95% CI) (months) | 11.7 (9.66 to 13.27) | 13.8 (11.01 to 15.87) |
| Hazard ratio (95% CI) | 0.812 (0.634 to 1.042) | |
| Median PFS (95% CI) (months) | 3.9 (3.02 to 4.30) | 6.7 (5.72 to 8.21) |
| Hazard ratio (95% CI) | 0.645 (0.498 to 0.835) | |
| Patients with no prior bevacizumab excluding adjuvant only (n (%)) | 371 (67.5%) | 375 (67.9%) |
| Median overall survival (95% CI) (months) | 12.4 (11.17 to 13.54) | 13.7 (12.71 to 16.03) |
| Hazard ratio (95% CI) | 0.766 (0.645 to 0.908) | |
| Median PFS (95% CI) (months) | 5.3 (4.50 to 5.55) | 6.9 (6.24 to 7.20) |
| Hazard ratio (95% CI) | 0.777 (0.655 to 0.921) | |
a As determined per IVRS
b OS in ITT population excluding patients who progressed during or within 6 months of adjuvant therapy demonstrated an HR (95% CI) of 0.78 (0.68 to 0.90) [median OS (95% CI) with Placebo/FOLFIRI 11.9 months (10.88 to 13.01) and with ZALTRAP/FOLFIRI 13.8 months (12.68 to 15.44)]
Other subgroup analyses for overall survival and progression free survival according to age (<65; ≥65), gender, presence of liver metastasis only, history of prior hypertension, and number of organs involved, showed a treatment effect favouring the ZALTRAP/FOLFIRI regimen over the placebo/FOLFIRI regimen.
In sub-group analysis of overall survival, a benefit consistent with the overall population was observed in patients <65 years old and ≥65 years old who received the ZALTRAP/FOLFIRI regimen.
Exploratory biomarker analyses were undertaken in the VELOUR trial including analyses of RAS mutational status in 482 of 1,226 patients (n=240 aflibercept; 242 placebo). In patients with RAS wild type tumours the HR (95% CI) for OS was 0.7 (0.5-1.0) with a median OS of 16.0 months for patients treated with aflibercept, and 11.7 months for the patients treated with placebo. Corresponding data in patients with RAS mutant type tumours showed a HR for OS of 0.9 (0.7-1.2) with median 12.6 and 11.2 months for aflibercept and placebo, respectively. These data are exploratory and the statistical interaction test was non-significant (lack of evidence for heterogeneity in treatment effect between the RAS wild-type and RAS mutant subgroups).
Paediatric population
The European Medicines Agency has waived the obligation to conduct studies with ZALTRAP in all subsets of the paediatric population in adenocarcinoma of the colon and rectum (see section 4.2 for information on paediatric use).
Pharmacokinetic properties
The pharmacokinetic properties described below have to a large extent been derived from a population pharmacokinetic analysis with data from 1,507 patients with various types of advanced malignancies.
Absorption
In preclinical tumour models, biologically active doses of aflibercept correlated with those necessary to produce circulating concentrations of free aflibercept in excess of VEGF-bound aflibercept. Circulating concentrations of VEGF-bound aflibercept increase with the aflibercept dose until most available VEGF is bound. Further increases in the aflibercept dose resulted in dose-related increases in circulating free aflibercept concentrations but only small further increases in the VEGF-bound aflibercept concentration.
In patients, ZALTRAP is administered at the dose of 4 mg/kg intravenously every two weeks for which there is an excess of circulating free aflibercept compared to VEGF-bound aflibercept.
At the recommended dose regimen of 4 mg/kg every two weeks, concentration of free aflibercept were near steady-state levels by the second cycle of treatment with essentially no accumulation (accumulation ratio of 1.2 at steady-state compared to the first administration).
Distribution
The volume of distribution of free aflibercept at steady-state is approximately 8 litres.
Biotransformation
No metabolism studies have been conducted with aflibercept since it is a protein. Aflibercept is expected to degrade to small peptides and individual amino acids.
Elimination
Free aflibercept is primarily cleared by binding to endogenous VEGF to form a stable, inactive complex. As with other large proteins, both free and bound aflibercept, are expected to be cleared, more slowly, by other biological mechanisms, such as proteolytic catabolism.
At doses greater than 2 mg/kg, free aflibercept clearance was approximately 1.0 L/day with a terminal half-life of 6 days.
High molecular weight proteins are not cleared by the renal route, therefore renal elimination of aflibercept is expected to be minimal.
Linearity/non-linearity
Consistent with target-mediated drug disposition, free aflibercept exhibits a faster (non-linear) clearance at doses below 2 mg/kg, likely due to the high affinity binding of aflibercept to endogenous VEGF. Linear clearance observed in the dose range of 2 to 9 mg/kg is likely due to non saturable biological mechanisms of elimination such as protein catabolism.
Other special populations
Elderly
There was no effect of age on the pharmacokinetics of free aflibercept.
Race
No effect of race was identified in the population analysis.
Gender
Gender was the most significant covariate for explaining the interindividual variability of free aflibercept clearance and volume with a 15.5% higher clearance and a 20.6% higher volume of distribution in males than in females. These differences do not affect exposure due to weight-based dosing and no dose modifications based on gender are required.
Weight
Weight had an effect on free aflibercept clearance and volume of distribution resulting with a 29% increase in aflibercept exposure in patients weighing ≥100 kg.
Hepatic impairment
There have been no formal studies with ZALTRAP in patients with hepatic impairment. In a population pharmacokinetic analysis with data from 1,507 patients with various types of advanced malignancies receiving ZALTRAP with or without chemotherapy, 63 patients with mild hepatic impairment (total bilirubin >1.0 x – 1.5 x ULN and any AST) and 5 patients with moderate hepatic impairment (total bilirubin >1.5 x – 3 x ULN and any AST) were treated with ZALTRAP. In these mild and moderate hepatic impairment patients, there was no effect on clearance of aflibercept. There are no data available for patients with severe hepatic impairment (total bilirubin >3 x ULN and any AST).
Renal impairment
There have been no formal studies with ZALTRAP in patients with renal impairment. A population pharmacokinetic analysis was conducted with data from 1,507 patients with various types of advanced malignancies receiving ZALTRAP with or without chemotherapy. This population included; 549 patients with mild renal impairment (CLCR between 50-80 ml/min), 96 patients with moderate renal impairment (CLCR between 30-50 ml/min), and 5 patients with severe renal impairment (CLCR <30 ml/min). This population pharmacokinetic analysis revealed no clinically meaningful differences in clearance or systemic exposure (AUC) of free aflibercept in patients with moderate and mild renal impairment at the 4 mg/kg dose of ZALTRAP as compared to the overall population studied. No conclusion can be drawn for patients with severe renal impairment due to very limited data available. In the few patients with severe renal impairment, drug exposure was similar to that observed in patients with normal renal function.
Preclinical safety data
Animal toxicology and pharmacology
Weekly/every two weeks intravenous administration of aflibercept to cynomolgus monkeys for up to 6 months resulted in changes in the bone (effects on growth plate and the axial and appendicular skeleton), nasal cavity, kidney, ovary, and adrenal gland. Most aflibercept-related findings were noted from the lowest dose tested corresponding to plasma exposures close to those in patients at the therapeutic dose. Most aflibercept-induced effects were reversible after a 5-month drug free period with the exception of skeletal and nasal cavity findings. Most findings were considered to be related to the pharmacological activity of aflibercept.
Aflibercept administration resulted in a delay in wound healing in rabbits. In full-thickness excisional and incisional skin wound models, aflibercept administration reduced fibrous response, neovascularisation, epidermal hyperplasia/re-epithelialisation, and tensile strength. Aflibercept increased blood pressure in normotensive rodents.
Carcinogenesis and mutagenesis
No studies have been conducted to evaluate carcinogenicity or mutagenicity of aflibercept.
Impairment of fertility
No specific studies with aflibercept have been conducted in animals to evaluate the effect on fertility. However, results from a repeat dose toxicity study suggest there is a potential for aflibercept to impair reproductive function and fertility. In sexually mature female cynomolgus monkeys inhibition of ovarian function and follicular development was evidenced. These animals also lost normal menstrual cycling. In sexually mature male cynomolgus monkeys a decrease in sperm motility and an increase in incidence of morphological abnormalities of spermatozoa were observed. There was no margin of exposure to patients in relation to these effects. These effects were fully reversible within 8-18 weeks after the last injection.
Reproductive and developmental toxicology
Aflibercept has been shown to be embryotoxic and teratogenic when administered intravenously to pregnant rabbits every 3 days during the organogenesis period (gestation days 6 to18) at doses approximately 1 to 15 times the human dose of 4 mg/kg every 2 weeks. Observed effects included 23 decreases in maternal body weights, an increased number of foetal resorptions, and an increased incidence of external, visceral, and skeletal foetal malformations.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.