Dalbavancin
Chemical formula: C₈₈H₁₀₀Cl₂N₁₀O₂₈ Molecular mass: 1,814.609 g/mol PubChem compound: 23724878
Mechanism of action
Dalbavancin is a bactericidal lipoglycopeptide. Its mechanism of action in susceptible Gram-positive bacteria involves interruption of cell wall synthesis by binding to the terminal D-alanyl-D-alanine of the stem peptide in nascent cell wall peptidoglycan, preventing cross-linking (transpeptidation and transglycosylation) of disaccharide subunits resulting in bacterial cell death.
Pharmacodynamic properties
Mechanism of resistance
All Gram-negative bacteria are inherently resistant to dalbavancin.
Resistance to dalbavancin in Staphylococcus spp. and Enterococcus spp. is mediated by VanA, a genotype that results in modification of the target peptide in nascent cell wall. Based on in vitro studies the activity of dalbavancin is not affected by other classes of vancomycin resistance genes.
Dalbavancin MICs are higher for vancomycin-intermediate staphylococci (VISA) than for fully vancomycin susceptible strains. If the isolates with higher dalbavancin MICs represent stable phenotypes and are correlated with resistance to the other glycopeptides, then the likely mechanism would be an increase in the number of glycopeptide targets in nascent peptidoglycan.
Cross-resistance between dalbavancin and other classes of antibiotics was not seen in in vitro studies. Methicillin resistance has no impact on dalbavancin activity.
Interactions with other antibacterial agents
In in vitro studies, no antagonism has been observed between dalbavancin and other commonly used antibiotics (i.e. cefepime, ceftazidime, ceftriaxone, imipenem, meropenem, amikacin, aztreonam, ciprofloxacin, piperacillin/tazobactam and trimethoprim/sulfamethoxazole), when tested against 12 species of Gram-negative pathogens.
PK/PD relationship
Bactericidal activity against staphylococci in vitro is time-dependent at serum concentrations of dalbavancin similar to those obtained at the recommended dose in humans. In vivo PK/PD relationship of dalbavancin for S. aureus was investigated using a neutropenic model of animal infection. This showed that the antibacterial activity of dalbavancin appears to best correlate with the ratio of area under the unbound plasma concentration-time curve to minimal inhibitory concentration (fAUC/MIC).
Clinical efficacy against specific pathogens
Efficacy has been demonstrated in clinical studies against the pathogens listed for ABSSSI that were susceptible to dalbavancin in vitro:
- Staphylococcus aureus,
- Streptococcus pyogenes,
- Streptococcus agalactiae,
- Streptococcus dysgalactiae,
- Streptococcus anginosus group (includes S. anginosus, S. intermedius, and S. constellatus).
Antibacterial activity against other relevant pathogens
Clinical efficacy has not been established against the following pathogens although in vitro studies suggest that they would be susceptible to dalbavancin in the absence of acquired mechanisms of resistance:
- Group G streptococci,
- Clostridium perfringens,
- Peptostreptococcus spp.
Pharmacokinetic properties
The pharmacokinetics of dalbavancin have been characterised in healthy subjects, patients, and special populations. Systemic exposures to dalbavancin are dose proportional following single doses over a range of 140 to 1120 mg, indicating linear pharmacokinetics of dalbavancin. No accumulation of dalbavancin was observed following multiple intravenous infusions administered once-weekly for up to 8 weeks (1 000 mg on Day 1, followed by up to 7 weekly 500 mg doses) in healthy adults.
The mean terminal elimination half-life (t1/2) was 372 (range 333 to 405) hours. The pharmacokinetics of dalbavancin are best described using a three-compartment model (α and β distributional phases followed by a terminal elimination phase). Thus, the distributional half-life (t1/2β), which constitutes most of the clinically-relevant concentration-time profile, ranged from 5 to 7 days and is consistent with once-weekly dosing.
Estimated pharmacokinetic parameters of dalbavancin following the two-dose regimen and the single-dose regimen, respectively, are shown in Table 1 below.
Table 1. Mean (SD) dalbavancin pharmacokinetic parameters using population PK analysis1:
| Parameter | Two-dose regimen2 | Single-dose regimen3 |
|---|---|---|
| Cmax (mg/L) | Day 1: 281 (52) Day 8: 141 (26) | Day 1: 411 (86) |
| AUC0-Day14 (mg•h/L) | 18100 (4600) | 20300 (5300) |
| CL (L/h) | 0.048 (0.0086) | 0.049 (0.0096) |
1 Source: DAL-MS-01.
2 1 000 mg on Day 1 + 500 mg on Day 8; Study DUR001-303 subjects with evaluable PK sample.
3 1 500 mg; Study DUR001-303 subjects with evaluable PK sample.
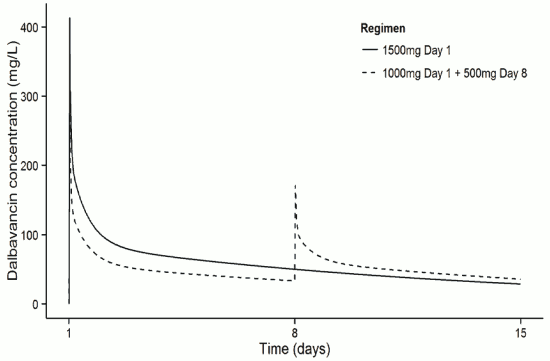
The dalbavancin plasma concentration-time following the two-dose and the single-dose regimens, respectively, are shown in Figure 1.
Figure 1. Dalbavancin Plasma Concentrations versus time in a typical adult ABSSSI patient (simulation using population pharmacokinetic model) for both the single and the two-dose regimens:
Distribution
Clearance and volume of distribution at steady state are comparable between healthy subjects and patients with infections. The volume of distribution at steady state was similar to the volume of extracellular fluid. Dalbavancin is reversibly bound to human plasma proteins, primarily to albumin. The plasma protein binding of dalbavancin is 93% and is not altered as a function of drug concentration, renal insufficiency, or hepatic insufficiency. Following a single intravenous dose of 1 000 mg in healthy volunteers AUC in skin blister fluid amounted (bound and unbound dalbavancin) to approximately 60% of the plasma AUC at day 7 post-dose.
Biotransformation
Metabolites have not been observed in significant amounts in human plasma. The metabolites hydroxy-dalbavancin and mannosyl aglycone have been detected in urine (<25% of administered dose). The metabolic pathways responsible for producing these metabolites have not been identified; however, due to the relatively minor contribution of metabolism to the overall elimination of dalbavancin, drug-drug interactions via inhibition or induction of metabolism of dalbavancin are not anticipated. Hydroxy-dalbavancin and mannosyl aglycone show significantly less antibacterial activity compared to dalbavancin.
Elimination
Following administration of a single 1 000 mg dose in healthy subjects, an average of 19% to 33% of the administered dalbavancin dose was excreted in urine as dalbavancin and 8% to 12% as the metabolite hydroxy-dalbavancin. Approximately 20% of the administered dose was excreted in faeces.
Special populations
Renal impairment
The pharmacokinetics of dalbavancin were evaluated in 28 adult subjects with varying degrees of renal impairment and in 15 matched control subjects with normal renal function. Following a single dose of 500 mg or 1 000 mg dalbavancin, the mean plasma clearance (CLT) was reduced 11%, 35%, and 47% in subjects with mild (CLCR 50-79 ml/min), moderate (CLCR 30–49 ml/min), and severe (CLCR <30 ml/min) renal impairment, respectively, compared to subjects with normal renal function. The mean AUC for subjects with creatinine clearance <30 ml/min was approximately 2-fold higher. The clinical significance of the decrease in mean plasma CLT, and the associated increase in AUC0-∞ noted in these pharmacokinetic studies of dalbavancin in subjects with severe renal impairment has not been established. Dalbavancin pharmacokinetics in subjects with end-stage renal disease receiving regularly scheduled renal dialysis (3 times/week) were similar to those observed in subjects with mild to moderate renal impairment, and less than 6% of an administered dose is removed after 3 hours of haemodialysis. For dosing instructions in adult subjects with renal impairment refer to section 4.2.
There is insufficient information to recommend dose adjustment for patients 3 months to 18 years with creatinine clearance less than 30 mL/min/1.73 m². Patients <3 months old with renal impairment, defined as serum creatinine ≥2 times the upper limit of normal, or urine output <0.5 mL/kg/h, or requirement for dialysis, were excluded from the clinical trials. For the 18 paediatric patients <3 months old that were included in the clinical trials, the range of normalised creatinine clearance (based on Schwartz bedside equation) was 34 to 118 mL/min/1.73 m². No observed PK data are available in paediatric patients with severe renal impairment. The predicted dalbavancin mean AUC for paediatric subjects with severe renal impairment (CLCR ≤30 ml/min/1.73 m²) was approximately 13-30% higher compared to paediatric patients with normal renal function treated with the same dose, based on population pharmacokinetic modelling.
Hepatic impairment
The pharmacokinetics of dalbavancin were evaluated in 17 subjects with mild, moderate, or severe hepatic impairment and compared to 9 matched healthy subjects with normal hepatic function. The mean AUC was unchanged in subjects with mild hepatic impairment compared to subjects with normal hepatic function; however, the mean AUC decreased by 28% and 31%, respectively, in subjects with moderate and severe hepatic impairment. The cause and the clinical significance of the decreased exposure in subjects with moderate and severe hepatic function are unknown. For dosing instructions in subjects with hepatic impairment refer to section 4.2.
Gender
Clinically significant gender-related differences in dalbavancin pharmacokinetics have not been observed in healthy subjects or in patients with infections. No dose adjustment is recommended based on gender.
Elderly
The pharmacokinetics of dalbavancin were not significantly altered with age; therefore, dose adjustment is not necessary based on age (see section 4.2). The experience with dalbavancin in elderly is limited: 276 patients ≥75 years of age were included in the Phase ⅔ clinical studies, of which 173 received dalbavancin. Patients up to 93 years of age have been included in clinical studies.
Paediatric population
The pharmacokinetics of dalbavancin has been evaluated in 219 paediatric patients [4 days to 17 years of age, including preterm neonates (gestational age 32 to <37 weeks; n=3) and term neonates (gestational age 37 to 40 weeks; n=5)]. The model predicted mean plasma AUC0-120h of dalbavancin in preterm neonates at birth (gestational age 32 weeks to <37 weeks) was approximately 62% of that in adult patients, whereas the AUC0-120h in older paediatric groups was 84-96% of that in adult patients. However, in all paediatric age groups, the percentage of patients attaining the PK/PD targets related to the in vivo drug activity were above 90% for MICs up to 0.5 mg/L.
Table 2. Simulated Mean (SD) dalbavancin pharmacokinetic parameters for paediatrics and adults using population PK analysis1:
| Parameter | Preterm Neonate | Term Neonate | Young Infant | Infant | Toddler | Child | Adolescent | Adult |
|---|---|---|---|---|---|---|---|---|
| Age range | GA 26 - <37 weeks | Birth - 1 month | 1 month - <3 months | 3 months - <2 years | 2 years - <6 years | 6 years - <12 years | 12 years - <18 years | ≥18 years |
| Dose | 22.5 mg/kg | 22.5 mg/kg | 22.5 mg/kg | 22.5 mg/kg | 22.5 mg/kg | 18 mg/kg | 18 mg/kg | 1500 mg |
| Cmax (mg/L) | 228 (88) | 305 (130) | 305 (130) | 306 (130) | 303 (130) | 258 (110) | 250 (110) | 417 (110) |
| AUC0-120h (mg•h/L) | 6 480 (2 000) | 8 930 (2 900) | 9 040 (3 000) | 9 470 (3 100) | 10 100 (3 300) | 8 850 (2 900) | 9 030 (3 100) | 10 500 (3 100) |
1 Source: DAL-MS-03.
Preclinical safety data
Dalbavancin toxicity has been evaluated after daily intravenous administration for durations of up to 3 months in rats and dogs. Dose-dependent toxicity included serum chemistry and histological evidence of renal and hepatic injury, reduced red blood cell parameters and injection site irritation. In dogs only, infusion reactions characterised by skin swelling and/or redness (not associated with the injection site), mucosal pallor, salivation, vomiting, sedation, and modest declines in blood pressure and increases in heart rate were observed in a dose-dependent manner. These infusion reactions were transient (resolved within 1 hour post-dosing) and were attributed to histamine release. Dalbavancin toxicity profile in juvenile rats was consistent with that previously observed in adult rats at the same dose (mg/kg/day) levels.
Reproductive toxicity studies in rats and rabbits showed no evidence of a teratogenic effect. In rats, at exposures approximately 3 times above clinical exposure, there was reduced fertility and an increased incidence of embryo-lethality, reductions in foetal weight and skeletal ossification and increased neonatal mortality. In rabbits, abortion occurred in conjunction with maternal toxicity at exposures below the human therapeutic range.
Long-term carcinogenicity studies have not been conducted. Dalbavancin was not mutagenic or clastogenic in a battery of in vitro and in vivo genotoxicity tests.
Related medicines
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.