Chemical formula: C₂₀H₁₉N₅ Molecular mass: 329.398 g/mol PubChem compound: 214347
Dapivirine is an NNRTI with potent antiviral activity against HIV-1. It prevents viral replication by binding directly to HIV-1 reverse transcriptase (RT) and blocking its activity. Dapivirine binding is non-competitive against both the RNA template and the nucleotide substrate.
In vitro studies have shown that dapivirine inhibits HIV-1 replication with EC50 values ranging from 0,9 nM (0,3 ng/mL) to 12 nM (3,9 ng/mL) for laboratory isolates and from <0,5 nM (0,2 ng/mL) to 2,6 nM (0,9 ng/mL) in clinical isolates from HIV-1 subtypes CRF02_AG, B, C, D, CRF05_DF, H, CRF01_AE, and G.
Dapivirine has been shown to prevent HIV- 1 infection of susceptible cells when present during viral exposure using monocyte-derived dendritic cells and autologous CD4+ T-cells. In human ectocervical tissue explants >99% inhibition of HIV-1BaL infection was observed at concentrations ≥10 nM (3,3 ng/mL), and transfer of free virus by migratory dendritic cells to indicator T-cells was blocked at 100 nM (32,9 ng/mL). Pre-treatment with 10 µM (3,3 µg/mL) dapivirine for 2 or 24 hours inhibited HIV-1 infection and virus dissemination by migratory cells for up to 6 days.
The activity of dapivirine is not significantly changed in the presence of semen and cervical mucus. In vivo studies have shown that dapivirine inhibits infection in humanised severe combined immunodeficient (hu-SCID) mouse model when mice were challenged vaginally with HIV-1.
In vitro susceptibility tests on HIV-1 isolates encoding one or more known NNRTI resistance mutations showed EC50 values of less than 100 nM (33 ng/mL) for 80 % of tested isolates. Selection of dapivirine-resistant strains occurs in vitro, with some strains requiring more than one substitution in the reverse transcriptase gene. The most frequently observed mutation during in vitro passage experiments is Y181C.
In analyses of dapivirine susceptibility, the following mutations showed a fold-change in susceptibility of >2 – ≤10: A98G, L100V, K101E, K103S, V106A, E138A/K/Q, Y181L; a >10 - ≤100 fold-change was observed for: L100I, K103N, Y181C, G190Q, F227C and M230I/L; a >100 fold-change was observed for: K101P, E138R, Y181I/V, Y188L and G190E. Multiple NNRTI mutations yielded increased susceptibility reduction with a >100 fold-change observed for double mutants: L100I+K103N, K103N+Y181C, V106A+F227C, E138A+F227C and Y181C+F227C. Mutations observed in Phase III trials IPM 027 and MTN-020 included A98G, K101E, K103N, E138A, G190G/A, H221Y, K101E+E138A, K101E+E138G, K103S+V106M, V108V/I+E138A, E138A+V179D, E138A+V179I/T, K103K/N+V106V/M. An analysis of dapivirine susceptibility in viruses without genotypic mixtures showed 0,5 – 19,3-fold-change (geometric mean: IPM 027: 3,06; MTN-020: 3,29).
The Phase III trials were performed in sub-Saharan Africa, where subtype C virus is the most common subtype. In these trials, a low and similar proportion of women in both dapivirine vaginal ring and placebo ring groups had NNRTI mutations identified in samples taken soon after HIV-1 infection (IPM 027: dapivirine vaginal ring : 16/84, 19,0%; placebo ring: 8/58, 13,8%; MTN-020: dapivirine vaginal ring : 8/68, 11,8%; placebo ring: 9/96, 9,4%).
The most prevalent mutation observed in these trials was the E138A variant, with a higher proportion of participants who had virus with this variant noted in the dapivirine vaginal ring group in one Phase III trial (IPM 027 trial) (11,9% [10/84]) compared to the placebo group (3,4% [2/58]; P=0,12, Fishers Exact Test), while no difference between treatment groups was observed in the other Phase III trial (MTN-020, 4,4% [3/68] vs 5,2% [5/96]). The E138A variant is a known polymorphism reported to have been observed in up to 8% of antiretroviral-naïve subtype C HIV-1 infected patients. The most frequently observed mutation during in vitro passage experiment, Y181C, was not observed in any dapivirine vaginal ring -exposed participants in either of the Phase III clinical trials. Five participants in the dapivirine vaginal ring group in IPM 027 had HIV-1 infection prior to enrolment. Four participants had genotypic testing at enrolment, seroconversion and Exit visits. Virus from one participant had E138A throughout. None had a change of genotype at seroconversion or the Exit visit.
In the IPM 027 trial the proportion of participants with more than one NNRTI resistance-associated mutation was comparable between the dapivirine vaginal ring group and the placebo ring group. There were more participants with more than one NNRTI resistance-associated mutation in the dapivirine vaginal ring group in the MTN-020 trial (7,3% [5/68] of participants in the dapivirine vaginal ring group and 1 % [1/96] of participants in the placebo ring group). In virus of three of the five participants, one of the mutations was the E138A polymorphism.
The mechanism by which differences between treatment groups arose is not clear (i.e. whether through passive transmission of resistant variants or active selection pressure through use of the dapivirine vaginal ring).
In general, genotypic analyses indicated that high level resistance to the NNRTIs efavirenz and nevirapine, commonly used in the treatment of HIV/AIDS, was infrequent in both treatment groups. Phenotypic analysis of virus with the E138A substitution indicated that full susceptibility or only small reductions in susceptibility to other NNRTIs occurred in these viruses from both the dapivirine vaginal ring and placebo ring groups.
Exposure to dapivirine following HIV-1 infection was limited and no conclusions can be drawn regarding the risk of resistance emerging with longer-term exposure to the dapivirine vaginal ring in an HIV-1 infected woman.
NNRTI resistance associated mutations observed in the open-label extension trials (IPM 032 and MTN-025) were consistent with those observed in the Phase III trials. These mutations included A98G, K101E, K103N, E138A, E138A with V179D and V106M with V179D. A higher proportion of NNRTI mutations was observed in the open label trials (IPM 032: 5/17, 29,4% and MTN-025: 6/33, 18,2%) compared to the pivotal trial IPM 027 (16/84; 19,0%).
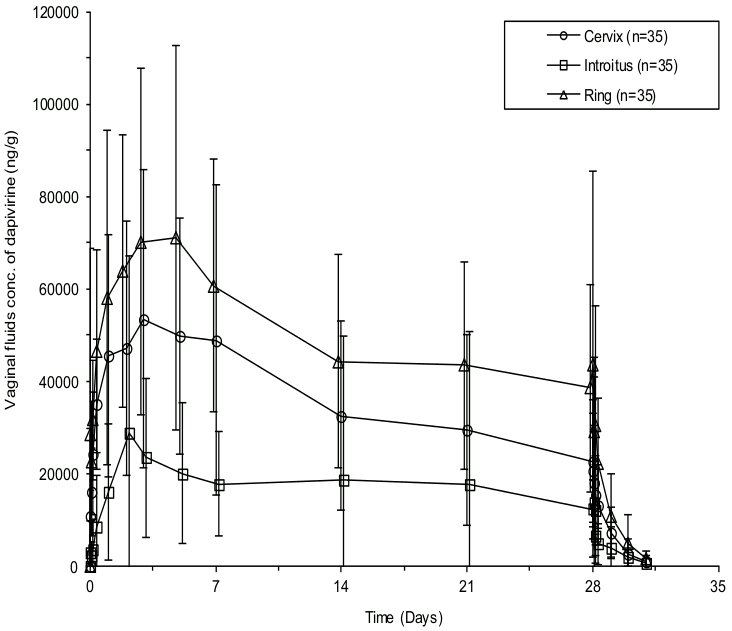
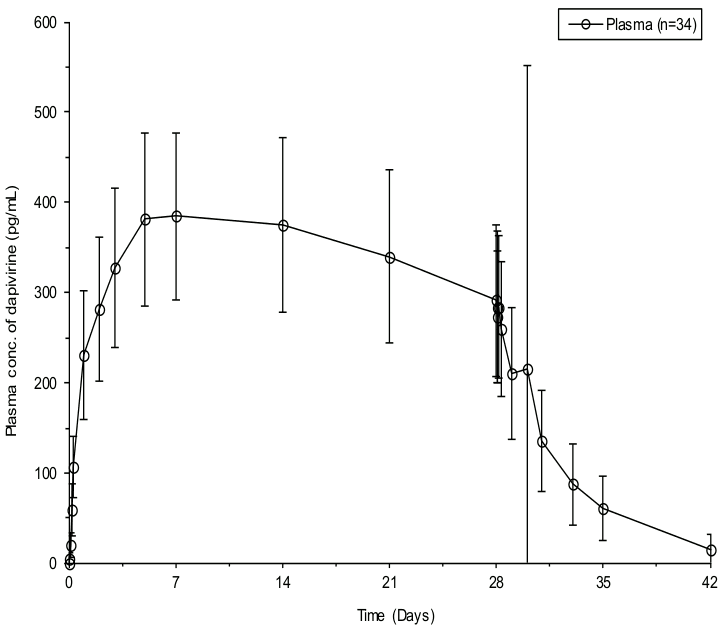
Dapivirine is released from the ring in a sustained manner, distributed into vaginal fluid and absorbed into surrounding tissues and plasma. Measurable dapivirine concentrations were detected in vaginal fluid and plasma within 1 to 4 hours after ring insertion (Figure 1A and 1B). Concentrations of dapivirine in vaginal fluid exceeding the in vitro HIV-1 IC99 by 1000-fold are achieved within 24 hours of ring insertion. At 4 to 24 hours after ring insertion, vaginal fluid concentrations (at all 3 sampling locations: cervix, ring area and introïtus) are similar to those on Day 28 after continuous ring use. Dapivirine plasma concentrations at 24 hours after ring insertion are also similar to those at 28 days after continuous ring use. Systemic concentrations of dapivirine observed in plasma with the use of the dapivirine vaginal ring were low (<2 ng/mL). Pharmacokinetic parameters in vaginal fluid (cervix) and plasma are summarised in the table below.
Figure 1A. Mean (SD) dapivirine concentrations in vaginal fluid following continuous use of the dapivirine vaginal ring for 28 days and after removal of the ring on day 28 (IPM 028):
Figure 1B. Mean (SD) dapivirine concentrations in plasma following continuous use of the dapivirine vaginal ring for 28 days and after removal of the ring on day 28 (IPM 028):
Dapivirine pharmacokinetic parameters in vaginal fluid (cervix) and plasma during use of the dapivirine vaginal ring for 28 days (IPM 028):
| PK Parameter | Plasma | Vaginal fluid (cervix) |
|---|---|---|
| Cmax | 462,0 (288,0) pg/mL | 76,9 (33,7) μg/g |
| Tmax | 167,90 (48,92 – 719,98) h | 72,10 (8,07 – 336,23) h |
| AUC0-28days | 229 408 (57 399) pg,h/mL | 24 222 (10 476) µg,h/g |
| Cday28 | 291,0 (83,4) pg/mL | 22,78 (13,16) µg/g |
| t½,term | 81,5 (21,8) h | 13,1 (6,5) h |
Values are mean (SD) for all parameters except Tmax which is median (minimum, maximum).
In cervicovaginal fluid, the in vitro protein binding of dapivirine is 15%. Dapivirine is highly bound to plasma proteins (>99,6%) in vitro. After vaginal administration of 14C-dapivirine to non-pregnant rats, concentrations of drug-related material were highest in the vaginal wall, followed by small intestine wall, large intestine wall, stomach wall, liver, cecum wall, and abdominal fat. Concentrations in other tissues were very low. In two clinical trials where cervical tissue biopsies were evaluated, the interindividual dapivirine concentrations in tissue after 28 days of using the dapivirine vaginal ring were highly variable (ranging from 46 – 12 900 ng/ml), with the lowest measured dapivirine concentration still 10 times the in vitro IC99 in cervical tissue. The distribution of dapivirine into compartments other than plasma and vaginal fluid (e.g., cerebrospinal fluid) has not been evaluated in humans.
In vitro experiments indicate that in the liver dapivirine primarily undergoes oxidative metabolism by cytochrome P450 (CYP450; primarily CYP3A and, to a lesser extent, by the CYP2C family), followed by glucuronidation by UGT1A and -2B isoenzymes. Dapivirine is a substrate of CYP1A1 and CYP3A4 enzymes, but is not a substrate of CYP1A2, CYP1B1, CYP2B6, CYP2C8 or CYP2C19, or of UGT1A1, UGT1A3, UGT1A4, UGT1A6, UGT1A7, UGT1A8, UGT1A9 or UGT2B7. In vitro studies in vaginal tissue suggest that CYP450-mediated metabolism also occurs in tissues at the site of application, but no evidence of glucuronidation was detected.
Dapivirine was not a substrate of drug transporters P-gp, BCRP, MRP1, MRP4, and ENT1 in vitro at concentrations observed in the vaginal fluid and had no inhibitory effects on the activity of these transporters at maximal vaginal concentrations and maximal plasma concentrations. In vitro dapivirine showed varying degrees of inhibition of CYP1A1, CYP1A2, CYP1B1, CYP2B6, CYP2C8, CYP2C9, CYP2C19, and CYP3A4.
At maximal plasma concentrations, dapivirine is not an inhibitor of UGT1A1, 1A3, 1A4, 1A6, 1A7, 1A8, 1A9 and 2B7. In vaginal tissue no UGT enzyme activity was detected. Dapivirine was not an inducer via AhR (CYP1A2), CAR (CYP2B6) and PXR (CYP3A4) at 0,3 μM (0,1 μg/mL).
In the overall clinical trial population, the terminal elimination half-life (t1/2) of dapivirine was approximately 13 hours in vaginal fluid (cervix) and approximately 82 hours in plasma. In clinical trials with orally administered dapivirine, dapivirine was shown to undergo negligible renal clearance.
No clinical trials in women with renal or hepatic impairment have been performed. In view of the low systemic exposure of dapivirine, hepatic impairment is not expected to affect dapivirine exposure or the safety profile. Similarly, based on low plasma concentrations and negligible renal clearance of dapivirine, renal impairment is not expected to affect dapivirine exposure or the safety profile.
The pharmacokinetics of the dapivirine vaginal ring have not been studied in children under the age of 15 years.
One clinical trial evaluated the mean dapivirine plasma concentration in adolescent girls aged 15–17 years. The mean dapivirine plasma concentrations in adolescents were comparable to the mean dapivirine plasma concentrations in adults.
One clinical trial evaluated the mean dapivirine plasma concentration in post-menopausal women aged 45–65 years. The mean dapivirine plasma concentrations in these women were comparable to the mean dapivirine plasma concentrations in women of reproductive age.
Clinical data suggest that dapivirine vaginal fluid and plasma concentrations were within the same range in Black and Caucasian women.
In the absence of a surrogate marker or model for risk reduction in HIV-1 infection acquired via vaginal intercourse, no in vitro-in vivo correlation studies or pharmacodynamic trials were performed.
Dapivirine activity in cervical tissue (99% inhibitory concentration [IC99] in vitro against HIV-1BaL = 3,3 ng/mL) is considered relevant for the risk reduction of HIV-1 infection via the genital route. However, accurate determination of dapivirine concentrations within the target tissues is difficult because of the uncertainty of where measured drug concentrations are actually located (e.g., on the tissue surface, in the dead keratinised cell layers, or in interstitial fluid and living target cells). Therefore, dapivirine levels in vaginal fluid were used to provide information on the local distribution and exposure to dapivirine. Dapivirine vaginal fluid concentrations exceed the in vitro cervical tissue IC99 (HIV-1BaL) by more than 1,000-fold within hours after ring insertion and by more than 3 000-fold within 24 hours after ring insertion, and these concentrations are maintained for at least 28 days during continuous ring use. After 28 days of ring use, dapivirine concentrations in vaginal fluid are still >3 000-fold (at the introïtus) and >6,000-fold (near the ring and the cervix) above the IC99.
The ex vivo capacity of the vaginal fluid to protect susceptible cells from infection upon challenge in vitro with HIV-1 was tested using vaginal fluid samples collected by cervicovaginal lavage after ring removal. Despite the dilution due to the lavage fluid and likely loss of drug due to possible precipitation of dapivirine in the lavage fluid and adsorption of dapivirine to the collection equipment, the vaginal fluid samples contained sufficient dapivirine to inhibit in vitro HIV infection by a mean of 89%.
Non-clinical data reveal no special hazard for women relevant to use of the dapivirine vaginal ring based on conventional studies of safety pharmacology, repeated dose toxicity, irritancy, genotoxicity, carcinogenic potential and toxicity to reproduction and development. No clinically relevant local or systemic findings were seen in rabbits following vaginal administration of dapivirine for up to 9 months, at exposures well in excess of maximum human vaginal exposure.
There were no findings in embryo-foetal development studies in rats and rabbits following vaginal administration of dapivirine at systemic exposures in excess of those in women using the dapivirine vaginal ring.
In oral embryo-foetal development studies, embryo-foetal toxicity (increased post-implantation loss, decreased foetal body weight, increased cardiac and skeletal malformations/anomalies, and reduction in skeletal ossification) was seen at maternally toxic doses in rats (more than 1 000-fold higher than those resulting from maximum human vaginal exposure, based on Cmax and AUC24h), but not in rabbits.
In a rat oral pre-and post-natal development study, effects on offspring body weight were associated with maternal reductions in body weight gain and food consumption. No effects were seen at an exposure more than 1 000-fold higher than that resulting from maximum human vaginal exposure (based on Cmax and AUC24h).
In a rat oral fertility study, increased post-implantation loss, decreased body weight and weight gain pre-mating and during the post-coitum period, and decreased fertility and conception were seen at high doses. No effects were seen at an exposure more than 1 000-fold higher than that resulting from maximum human vaginal exposure (based on Cmax and AUC24h).
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.