Chemical formula: C₁₈H₂₀FN₃O₄ Molecular mass: 361.368 g/mol PubChem compound: 4583
Ofloxacin interacts in the following cases:
Ofloxacin, like other fluoroquinolones, should be used with caution in patients receiving drugs known to prolong the QT interval (e.g. Class IA and III anti-arrhythmics, tricyclic antidepressants, macrolides, antipsychotics).
he infusion time for ofloxacin IV should not be less than 30 minutes for 200 mg. This is of particular importance when ofloxacin is administered concomitantly with drugs that can lead to a reduction in blood pressure or with barbiturate-containing anaesthetics. Generally, individual doses are to be given at approximately equal intervals.
It is recommended that a maximum daily dose of 400 mg of ofloxacin be not exceeded, because of possible reduction of excretion.
Ofloxacin should be used with caution in patients with impaired liver function, as liver damage may occur. Cases of fulminant hepatitis potentially leading to liver failure (including fatal cases) have been reported with fluoroquinolones. Patients should be advised to stop treatment and contact their doctor if signs and symptoms of hepatic disease develop such as anorexia, jaundice, dark urine, pruritus or tender abdomen.
In patients with impaired renal function, the following oral or I.V. dosages are recommended:
| Creatinine clearance | Unit dose mg* | Number/24h | Intervals h |
|---|---|---|---|
| 50–20 ml/min | 100–200 | 1 | 24 |
| <20 ml/min** | 100 | 1 | 24 |
| or haemodialysis | or | ||
| or peritoneal dialysis | 200 | 1 | 48 |
* According to indication or dose interval.
** The serum concentration of ofloxacin should be monitored in patients with severe renal impairment and dialysis patients.
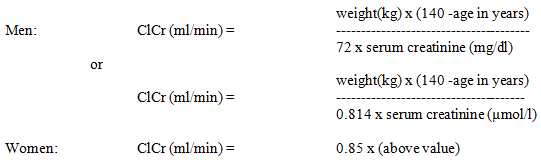
When creatinine clearance cannot be measured, it can be estimated with reference to the serum creatinine level using the following Cockcroft’s formula for adults:
Increased coagulation tests (PT/INR) and/or bleeding, which may be severe, have been reported in patients treated with ofloxacin in combination with a vitamin K antagonist (e.g. warfarin). Coagulation tests should be monitored in patients treated with vitamin K antagonists because of a possible increase in the effect of coumarin derivatives.
Ofloxacin may cause a slight increase in serum concentrations of glibenclamide administered concurrently; patients treated with this combination should be closely monitored.
Probenecid decreased the total clearance of ofloxacin by 24%, and increased AUC by 16%. The proposed mechanism is a competition or inhibition for active transport at the renal tubular excretion. Caution should be exercised when ofloxacin is co-administered with drugs that affect the tubular renal secretion such as probenecid, cimetidine, furosemide and methotrexate.
No pharmacokinetic interactions of ofloxacin were found with theophylline in a clinical study. However, a pronounced lowering of the cerebral seizure threshold may occur when quinolones are given concurrently with theophylline, nonsteroidal anti-inflammatory drugs, or other agents, which lower the seizure threshold.
Very rare cases of QT interval proplongation have been reported in patients taking fluoroquinolones.
Caution should be taken when using fluoroquinolones, including ofloxacin, in patients with known risk factors for prolongation of the QT interval such as, for example:
Psychotic reactions have been reported in patients receiving fluoroquinolones including ofloxacin. In some cases these have progressed to suicidal thoughts or self-endangering behavior including suicide attempt, sometimes after a single dose of ofloxacin. In the event that a patient develops these reactions, ofloxacin should be discontinued and appropriate measures instituted. Ofloxacin should be used with caution in patients with a history of psychotic disorder or in patients with psychiatric disease.
Tendonitis, rarely observed with quinolones, may occasionally lead to rupture involving Achilles tendon in particular. Tendinitis and tendon rupture, sometimes bilateral, may occur within 48 hours of starting treatment with ofloxacin and have been reported up to several months after discontinuation of ofloxacin. The risk of tendinitis and tendon rupture is increased in patients aged over 60 years and in patients using corticosteroids. The daily dose should be adjusted in elderly patients based on creatinine clearance. Close monitoring of these patients is therefore necessary if they are prescribed ofloxacin. All patients should consult their physician if they experience symptoms of tendinitis. If tendinitis is suspected, treatment with ofloxacin must be halted immediately, and appropriate treatment (e.g. immobilisation) must be initiated for the affected tendon.
Diarrhoea, especially if severe, persistent and/or bloody, occurring during or after treatment with ofloxacin (including several weeks after treatment), may indicate a condition caused by Clostridium difficile, the most severe form of which is pseudomembranous colitis (CDAD) CDAD may range in severity from mild to life threatening, the most severe form of which is pseudomembranous colitis. It is therefore important to consider this diagnosis in patients who develop serious diarrhoea during or after treatment with ofloxacin. If pseudo-membraneous colitis is suspected, treatment should be discontinued immediately.
Appropriate specific antibiotic therapy must be started without delay (e.g. oral vancomycin, oral teicoplanin or metronidazole). Medicinal products that inhibit peristalsis are contraindicated in such cases.
Cases of severe bullous skin reactions such as Stevens-Johnson syndrome or toxic epidermal necrolysis have been reported with ofloxacin. Patients should be advised to contact their doctor immediately prior to continuing treatment if skin and/or mucosal reactions occur.
Hypersensitivity and allergic reactions have been reported for fluoroquinolones after first administration. Anaphylactic and anaphylactoid reactions can progress to life-threatening shock, even after the first administration. In these cases ofloxacin should be discontinued and suitable treatment (e.g. treatment for shock) should be initiated.
As with all quinolones, disturbances in blood glucose, including both hypoglycaemia and hyperglycaemia have been reported, usually in diabetic patients receiving concomitant treatment with an oral hypoglycaemic agent (e.g. glibenclamide) or with insulin. Cases of hypoglycaemic coma have been reported. In these diabetic patients, careful monitoring of blood glucose is recommended.
Photosensitisation has been reported with ofloxacin. It is recommended that patients should not expose themselves unnecessarily to strong sunlight or to artificial UV rays (e.g. sunray lamp, solarium), during treatment and for 48 hours following treatment discontinuation in order to prevent photosensitisation.
Sensory or sensorimotor peripheral neuropathy has been reported in patients receiving fluoroquinolones, including ofloxacin, which can be rapid in its onset. Ofloxacin should be discontinued if the patient experiences symptoms of neuropathy. This would minimise the possible risk of developing an irreversible condition.
In case of convulsive seizures, treatment with ofloxacin should be discontinued.
Quinolones may lower the seizure threshold and may trigger seizures. Ofloxacin is contraindicated in patients with a history epilepsy or with a known predisposition to seizures. Patients with a known predisposition to seizures may include those with pre-existing central nervous system lesions, concomitant treatment with fenbufen and similar non-steroidal anti-inflammatory drugs (NSAIDs), or with drugs which lower the cerebral seizure threshold, such as theophylline. In case of convulsive seizures, treatment with ofloxacin should be discontinued.
Fluoroquinolones, including ofloxacin, have neuromuscular blocking activity and may exacerbate muscle weakness in patients with myasthenia gravis. Postmarketing serious adverse reactions, including deaths and the requirement for respiratory support, have been associated with fluoroquinolone use in patients with myasthenia gravis. Ofloxacin is not recommended in patients with a known history of myasthenia gravis.
Based on a limited amount of human data, the use of fluoroquinolones in the first trimester of pregnancy has not been associated with an increased risk of major malformations or other adverse effects on pregnancy outcome. Animal studies have shown damage to the joint cartilage in immature animals but no teratogenic effects. Therefore ofloxacin must not be used during pregnancy.
Ofloxacin is excreted into human breast milk in small amounts. Because of the potential for arthropathy and other serious toxicity in the nursing infant, breast-feeding should be discontinued during treatment with ofloxacin.
Since there have been occasional reports of drowsiness/somnolence, impairment of skills, dizziness/vertigo and visual disturbances, which may impair the patient’s ability to concentrate and react, and therefore may constitute a risk in situations where these abilities are of special importance (e.g. driving a car or operating machinery), patients should know how they react to ofloxacin before they drive or operate machinery. These effects may be enhanced by alcohol.
Common (≥1/100 to <1/10,000), Uncommon (≥1/1,000 to <1/100), Rare (≥1/10,000 to <1/1,000), Very rare (<1/10,000), Not known (cannot be estimated from available data)**
Uncommon: Fungal infection, Pathogen resistance
Very rare: Anaemia, Haemolytic anaemia, Leukopenia, Eosinophilia, Thrombocytopenia
Not known: Agranulocytosis, Bone marrow failure
Rare: Anaphylactic reaction**, Anaphylactoid reaction**, Angioedema**
Very rare: Anaphylactic shock**, Anaphylactoid shock**
Rare: Anorexia
Not known: Hypoglycaemia in diabetics treated with hypoglycaemic agents, Hyperglycaemia, Hypoglycaemic coma
Uncommon: Agitation, Sleep disorder, Insomnia
Rare: Psychotic disorder (for e.g. hallucination), Anxiety, Confusional state, Nightmares, Depression
Not known: Psychotic disorder and depression with self-endangering behaviour including suicidal ideation or suicide attempt, Nervousness
Uncommon: Dizziness, Headache
Rare: Somnolence, Paraesthesia, Dysgeusia, Parosmia
Very rare: Peripheral sensory neuropathy**, Peripheral sensory motor neuropathy**, Convulsion**, Extra-pyramidal symptoms or other disorders of muscular coordination
Not known: Tremor, Dyskinesia, Ageusia, Syncope, Benign intracranial hypertension (Pseudotumor cerebri)
Uncommon: Eye irritation
Rare: Visual disturbance
Not known: Uveitis
Uncommon: Vertigo
Very rare: Tinnitus, Hearing loss
Not known: Hearing impaired
Rare: Tachycardia
Not known: Ventricular arrhythmias, torsades de pointes (reported predominantly in patients with risk factors for QT prolongation), ECG QT prolonged
Common: applies only to the solution for infusion: Phlebitis
Rare: Hypotension
Not known: applies only to the solution for infusion: During infusion of ofloxacin, tachycardia and hypotension may occur. Such a decrease in blood pressure may, in very rare cases, be severe.
Uncommon: Cough, Nasopharyngitis
Rare: Dyspnoea, Bronchospasm
Not known: Allergic pneumonitis, Severe dyspnoea
Uncommon: Abdominal pain, Diarrhoea, Nausea, Vomiting
Rare: Enterocolitis, sometimes haemorrhagic
Very rare: Pseudo-membranous colitis*, Jaundice cholestatic
Not known: Dyspepsia, Flatulence, Constipation, Pancreatitis
Rare: Hepatic enzymes increased (ALAT, ASAT, LDH, gamma-GT and/or alkaline phosphatase), Blood bilirubin increased
Not known: Hepatitis, which may be severe**; Severe liver injury, including cases of acute liver failure, sometimes fatal, have been reported with ofloxacin, primarily in patients with underlying liver disorders
Uncommon: Pruritus, Rash
Rare: Urticaria, Hot flushes, Hyperhidrosis, Pustular rash
Very rare: Erythema multiforme, Toxic epidermal necrolysis, Photo-sensitivity reaction**, Drug eruption, Vascular purpura, Vasculitis, which can lead in exceptional cases to skin necrosis
Not known: Stevens-Johnson syndrome; Acute generalized exanthemous pustulosis; drug rash, Stomatitis; Exfoliative dermatitis
Rare: Tendonitis
Very rare: Arthralgia, Myalgia, Tendon rupture (e.g. Achilles tendon) which may occur within 48 hours of treatment start and may be bilateral.
Not known: Rhabdomyolysis and/or Myopathy, Muscular weakness, Muscle tear, muscle rupture, Ligament rupture, Arthritis
Rare: Serum creatinine increased
Very rare: Acute renal failure
Not known: Acute interstitial nephritis
Not known: Attacks of porphyria in patients with porphyria
Common: applies onlytothe solution for infusion: Infusion site reaction (pain, reddening)
Not known: Asthenia, Pyrexia, Pain (including pain in the back, chest and extremities)
* Very rare cases of prolonged (up to months or years), disabling and potentially irreversible serious drug reactions affecting several, sometimes multiple, system organ classes and senses (including reactions such as tendonitis, tendon rupture, arthralgia, pain in extremities, gait disturbance, neuropathies associated with paraesthesia, depression, fatigue, memory impairment, sleep disorders, and impairment of hearing, vision, taste and smell) have been reported in association with the use of quinolones and fluoroquinolones in some cases irrespective of pre-existing risk factors.
** postmarketing experience
Serious reactions after use of systemic ofloxacin are rare and most symptoms are reversible. Since a small amount of ofloxacin is systemically absorbed after topical administration, side-effects reported with systemic use could possibly occur.
Frequency categories: Very common (≥1/10); Common (≥1/100 to <1/10); Uncommon (≥1/1,000 to <1/100); Rare (≥1/10,000 to <1/1,000); Very rare (<1/10,000) and not known (cannot be estimated from the available data).
Not Known: Hypersensitivity reaction including signs or symptoms of Eye allergy (such as Eye pruritus and Eyelid pruritus) and Anaphylactic reactions (such as angioedema, dyspnea, anaphylactic shock, oropharyngeal swelling, facial oedema and tongue swollen)
Not known: Dizziness
Common: Eye irritation; Ocular discomfort
Not known: Keratitis; Conjunctivitis; Vision blurred; Photophobia; Eye oedema; Foreign body sensation in eyes; Lacrimation increased; Dry eye; Eye pain; Ocular hyperaemia; Periorbital oedema (including eyelid oedema)
Not known: ventricular arrhythmia and torsades de pointes (reported predominantly in patients with risk factors for QT prolongation); ECG QT prolonged
Not known: Nausea
Not Known: Stevens-Johnson syndrome; Toxic epidermal necrolysis
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.