Palonosetron
Chemical formula: C₁₉H₂₄N₂O Molecular mass: 296.414 g/mol PubChem compound: 6337614
Mechanism of action
Palonosetron competitively blocks the action of serotonin at 5-HT~3~ receptors located on vagal afferents in the chemoreceptor trigger zone (CTZ), resulting in suppression of chemotherapy-induced nausea and vomiting.
Pharmacodynamic properties
Palonosetron is a selective high-affinity receptor antagonist of the 5HT3 receptor.
Pharmacokinetic properties
Absorption
Intravenous administration
Following intravenous administration, an initial decline in plasma concentrations is followed by slow elimination from the body with a mean terminal elimination half-life of approximately 40 hours. Mean maximum plasma concentration (Cmax) and area under the concentration-time curve (AUC0-∞) are generally dose-proportional over the dose range of 0.3–90 μg/kg in healthy subjects and in cancer patients.
Following intravenous administration of palonosetron 0.25 mg once every other day for 3 doses in 11 testicular cancer patients, the mean (±SD) increase in plasma concentration from Day 1 to Day 5 was 42±34%. After intravenous administration of palonosetron 0.25 mg once daily for 3 days in 12 healthy subjects, the mean (±SD) increase in plasma palonosetron concentration from Day 1 to Day 3 was 110±45%.
Pharmacokinetic simulations indicate that the overall exposure (AUC0-∞) of 0.25 mg intravenous palonosetron administered once daily for 3 consecutive days was similar to a single intravenous dose of 0.75 mg, although Cmax of the 0.75 mg single dose was higher.
Oral administration
Following oral administration, palonosetron is well absorbed with its absolute bioavailability reaching 97%. After single oral doses using buffered solution mean maximum palonosetron concentrations (Cmax) and area under the concentration-time curve (AUC0-∞) were dose proportional over the dose range of 3.0 to 80 µg/kg in healthy subjects.
In 36 healthy male and female subjects given a single oral dose of palonosetron capsules 500 micrograms, maximum plasma palonosetron concentration (Cmax) was 0.81±0.17 ng/ml (mean±SD) and time to maximum concentration (Tmax) was 5.1±1.7 hours. In female subjects (n=18), the mean AUC was 35% higher and the mean Cmax was 26% higher than in male subjects (n=18). In 12 cancer patients given a single oral dose of palonosetron capsules 500 micrograms one hour prior to chemotherapy, Cmax was 0.93±0.34 ng/ml and Tmax was 5.1±5.9 hours. The AUC was 30% higher in cancer patients than in healthy subjects.
A high fat meal did not affect the Cmax and AUC of oral palonosetron. Therefore, palonosetron capsules may be taken without regard to meals.
Distribution
Palonosetron at the recommended dose is widely distributed in the body with a volume of distribution of approximately 6.9 to 7.9 l/kg. Approximately 62% of palonosetron is bound to plasma proteins.
Biotransformation
Palonosetron is eliminated by dual route, about 40% eliminated through the kidney and with approximately 50% metabolised to form two primary metabolites, which have less than 1% of the 5HT3 receptor antagonist activity of palonosetron. In vitro metabolism studies have shown that CYP2D6 and to a lesser extent, CYP3A4 and CYP1A2 isoenzymes are involved in the metabolism of palonosetron. However, clinical pharmacokinetic parameters are not significantly different between poor and extensive metabolisers of CYP2D6 substrates. Palonosetron does not inhibit or induce cytochrome P450 isoenzymes at clinically relevant concentrations.
Elimination
Intravenous administration
After a single intravenous dose of 10 micrograms/kg [14C]-palonosetron, approximately 80% of the dose was recovered within 144 hours in the urine with palonosetron representing approximately 40% of the administered dose, as unchanged active substance. After a single intravenous bolus administration in healthy subjects the total body clearance of palonosetron was 173±73 ml/min and renal clearance was 53±29 ml/min. The low total body clearance and large volume of distribution resulted in a terminal elimination half-life in plasma of approximately 40 hours. Ten percent of patients have a mean terminal elimination half-life greater than 100 hours.
Oral administration
Following administration of a single oral 750 micrograms dose of [14C]-palonosetron to six healthy subjects, 85% to 93% of the total radioactivity was excreted in urine, and 5% to 8% was eliminated in feces. The amount of unchanged palonosetron excreted in the urine represented approximately 40% of the administered dose. In healthy subjects given palonosetron capsules 500 micrograms, the terminal elimination half-life (t½) of palonosetron was 37±12 hours (mean±SD), and in cancer patients, t½ was 48±19 hours. After a single-dose of approximately 0.75 mg intravenous palonosetron, the total body clearance of palonosetron in healthy subjects was 160±35 ml/h/kg (mean±SD) and renal clearance was 66.5±18.2 ml/h/kg.
Pharmacokinetics in special populations
Elderly people
Age does not affect the pharmacokinetics of palonosetron. No dosage adjustment is necessary in elderly patients.
Gender
Gender does not affect the pharmacokinetics of palonosetron. No dosage adjustment is necessary based on gender.
Paediatric population
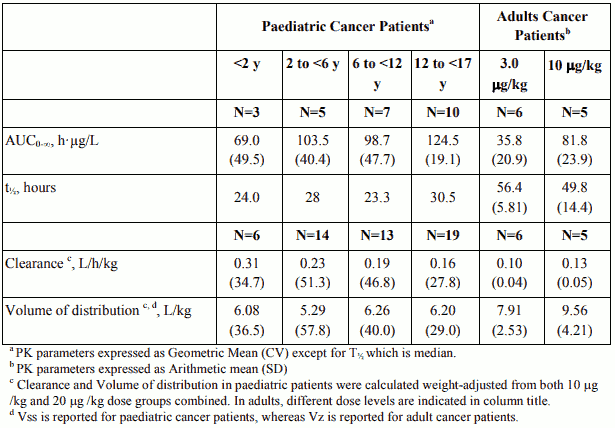
Single-dose i.v. palonosetron pharmacokinetic data was obtained from a subset of paediatric cancer patients (n=280) that received 10 µg/kg or 20 µg/kg. When the dose was increased from10 µg/kg to 20 µg/kg a dose-proportional increase in mean AUC was observed. Following single dose intravenous infusion of palonosetron 20 µg/kg, peak plasma concentrations (CT) reported at the end of the 15 minute infusion were highly variable in all age groups and tended to be lower in patients <6 years than in older paediatric patients. Median half-life was 29.5 hours in overall age groups and ranged from about 20 to 30 hours across age groups after administration of 20 µg/kg.
The total body clearance (L/h/kg) in patients 12 to 17 years old was similar to that in healthy adults. There are no apparent differences in volume of distribution when expressed as L/kg.
Pharmacokinetic Parameters in Paediatric Cancer Patients following intravenous infusion of palonosetron at 20 µg/kg over 15 min and in Adult Cancer Patients receiving 3 and 10 µg/kg palonosetron doses via intravenous bolus:
Renal impairment
Mild to moderate renal impairment does not significantly affect palonosetron pharmacokinetic parameters. Severe renal impairment reduces renal clearance, however total body clearance in these patients is similar to healthy subjects. No dosage adjustment is necessary in patients with renal insufficiency. No pharmacokinetic data in haemodialysis patients are available.
Hepatic impairment
Hepatic impairment does not significantly affect total body clearance of palonosetron compared to the healthy subjects. While the terminal elimination half-life and mean systemic exposure of palonosetron is increased in the subjects with severe hepatic impairment, this does not warrant dose reduction.
Preclinical safety data
Effects in non-clinical studies were observed only at exposures considered sufficiently in excess of the maximum human exposure indicating little relevance to clinical use.
Non-clinical studies indicate that palonosetron, only at very high concentrations, may block ion channels involved in ventricular de- and re-polarisation and prolong action potential duration.
Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/foetal development, parturition or postnatal development. Only limited data from animal studies are available regarding the placental transfer.
Palonosetron is not mutagenic. High doses of palonosetron (each dose causing at least 30 times the human therapeutic exposure) applied daily for two years caused an increased rate of liver tumours, endocrine neoplasms (in thyroid, pituitary, pancreas, adrenal medulla) and skin tumours in rats but not in mice. The underlying mechanisms are not fully understood, but because of the high doses employed and since palonosetron is intended for single application in humans, these findings are not considered relevant for clinical use.
Related medicines
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.