Source: FDA, National Drug Code (US) Revision Year: 2019
CAMBIA is a non-steroidal anti-inflammatory drug (NSAID). The mechanism of action of CAMBIA, like that of other NSAIDs, is not completely understood but may be related to prostaglandin synthetase inhibition.
Diclofenac is 100% absorbed after oral administration compared to intravenous administration as measured by urine recovery. However, due to first-pass metabolism, only about 50% of the absorbed dose is systemically available. In fasting volunteers, measurable plasma levels were observed within 5 minutes of dosing with CAMBIA. Peak plasma levels were achieved at approximately 0.25 hour in fasting normal volunteers, with a range of 0.17 to 0.67 hours. High fat food had no significant effect on the extent of diclofenac absorption, but there was a reduction in peak plasma levels of approximately 70% after a high fat meal. Decreased Cmax may be associated to decreased effectiveness.
The apparent volume of distribution (V/F) of diclofenac potassium is 1.3 L/kg.
Diclofenac is more than 99% bound to human serum proteins, primarily to albumin. Serum protein binding is constant over the concentration range (0.15-105 μg/mL) achieved with recommended doses.
Five diclofenac metabolites have been identified in human plasma and urine. The metabolites include 4'hydroxy, 5-hydroxy-, 3'hydroxy, 4',5-dihydroxy- and 3'-hydroxy-4'-methoxy diclofenac. The major diclofenac metabolite, 4'-hydroxydiclofenac, has very weak pharmacologic activity. The formation of 4'-hydroxy diclofenac is primarily mediated by CPY2C9. Both diclofenac and its oxidative metabolites undergo glucuronidation or sulfation followed by biliary excretion. Acylglucuronidation mediated by UGT2B7 and oxidation mediated by CPY2C8 may also play a role in diclofenac metabolism. CYP3A4 is responsible for the formation of minor metabolites, 5-hydroxy and 3'hydroxy diclofenac. In patients with renal impairment, peak concentrations of metabolites 4'-hydroxy-and 5- hydroxydiclofenac were approximately 50% and 4% of the parent compound after single oral dosing compared to 27% and 1% in normal healthy subjects.
Diclofenac is eliminated through metabolism and subsequent urinary and biliary excretion of the glucuronide and the sulfate conjugates of the metabolites. Little or no free unchanged diclofenac is excreted in the urine. Approximately 65% of the dose is excreted in the urine and approximately 35% in the bile as conjugates of unchanged diclofenac plus metabolites. Because renal elimination is not a significant pathway of elimination for unchanged diclofenac, dosing adjustment in patients with mild to moderate renal dysfunction is not necessary. The terminal half-life of unchanged diclofenac is approximately 2 hours.
There are no pharmacokinetic differences due to race.
The liver metabolizes almost 100% of diclofenac; there is insufficient information available to support dosing recommendations for CAMBIA in patients with hepatic insufficiency (5.3, 8.6)
In patients with renal impairment (inulin clearance 60-90, 30-60, and <30 mL/min; N=6 in each group), AUC values and elimination rate were comparable to those in healthy subjects.
Long term carcinogenicity studies in rats given diclofenac sodium up to 2 mg/kg/day (less than the recommended human dose [RHD] of 50 mg/day on a body surface area [mg/m²] basis) have revealed no significant increases in tumor incidence. There was a slight increase in benign mammary fibroadenomas in mid-dose treated (0.5 mg/kg/day or 3 mg/m²/day) female rats (high-dose females had excessive mortality), but the increase was not significant for this common rat tumor. A 2-year carcinogenicity study conducted in mice employing diclofenac sodium at doses up to 0.3 mg/kg/day (less than the RHD on a mg/m² basis) in males and 1 m/kg/day (less than the RHD on a mg/m² basis) in females did not reveal any oncogenic potential.
Diclofenac sodium was not genotoxic in in vitro (reverse mutation in bacteria [Ames], mouse lymphoma tk) or in in vivo (including dominant lethal and male germinal epithelial chromosomal aberration in Chinese hamster) assays.
Diclofenac sodium administered to male and female rats at 4 mg/kg/day (less than the RHD on a mg/m² basis) did not affect fertility.
The efficacy of CAMBIA in the acute treatment of migraine headache was demonstrated in two randomized, double-blind, placebo-controlled trials.
Patients enrolled in these two trials were predominantly female (85%) and white (86%), with a mean age of 40 years (range: 18 to 65). Patients were instructed to treat a migraine of moderate to severe pain with 1 dose of study medication. Patients evaluated their headache pain 2 hours later. Associated symptoms of nausea, photophobia, and phonophobia were also evaluated. In addition, the proportion of patients who were “sustained pain free”, defined as a reduction in headache severity from moderate or severe pain to no pain at 2 hours post-dose without a return of mild, moderate, or severe pain and no use of rescue medication for 24 hours post-dose, was also evaluated. In these studies, the percentage of patients achieving pain freedom 2 hours after treatment and sustained pain freedom from 2 to 24 hours post-dose was significantly greater in patients who received CAMBIA compared with those who received placebo (see Table 2). The percentage of patients achieving pain relief 2 hours after treatment (defined as a reduction in headache severity from moderate or severe pain to mild or no pain) was also significantly greater in patients who received CAMBIA compared with those who received placebo (see Table 2).
Table 2. Percentage of Patients With 2-Hour Pain Freedom, Sustained Pain Freedom 2-24 Hours, and 2-Hour Pain Relief Following Treatment:
| Study 1 | CAMBIA (n=265) | Placebo (n=257) |
|---|---|---|
| 2-Hour Pain Free | 24% | 13% |
| 2-24h Sustained Pain Free | 22% | 10% |
| 2-Hour Pain Relief | 48% | 27% |
| Study 2 | CAMBIA (n=343) | Placebo (n=347) |
| 2-Hour Pain Free | 25% | 10% |
| 2-24h Sustained Pain Free | 19% | 7% |
| 2-Hour Pain Relief | 65% | 41% |
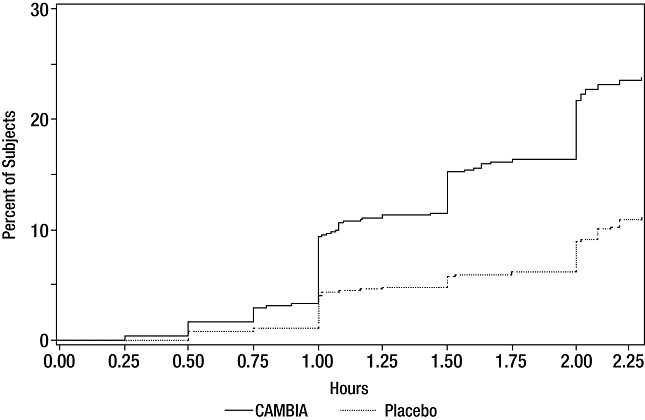
The estimated probability of achieving migraine headache pain freedom within 2 hours following treatment with CAMBIA is shown in Figure 1.
Figure 1. Percentage of Patients With Initial Headache Pain Freedom Within 2 Hours:
There was a decreased incidence of nausea, photophobia and phonophobia following administration of CAMBIA, compared to placebo. The efficacy and safety of CAMBIA was unaffected by age or gender of the patient.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.