CIPRO Film-coated tablet / Oral suspension kit Ref.[10545] Active ingredients: Ciprofloxacin
Source: FDA, National Drug Code (US) Revision Year: 2020
1. Indications and Usage
1.1 Skin and Skin Structure Infections
CIPRO is indicated in adult patients for treatment of skin and skin structure infections caused by Escherichia coli, Klebsiella pneumoniae, Enterobacter cloacae, Proteus mirabilis, Proteus vulgaris, Providencia stuartii, Morganella morganii, Citrobacter freundii, Pseudomonas aeruginosa, methicillin-susceptible Staphylococcus aureus, methicillin-susceptible Staphylococcus epidermidis, or Streptococcus pyogenes.
1.2 Bone and Joint Infections
CIPRO is indicated in adult patients for treatment of bone and joint infections caused by Enterobacter cloacae, Serratia marcescens, or Pseudomonas aeruginosa.
1.3 Complicated Intra-Abdominal Infections
CIPRO is indicated in adult patients for treatment of complicated intra-abdominal infections (used in combination with metronidazole) caused by Escherichia coli, Pseudomonas aeruginosa, Proteus mirabilis, Klebsiella pneumoniae, or Bacteroides fragilis.
1.4 Infectious Diarrhea
CIPRO is indicated in adult patients for treatment of infectious diarrhea caused by Escherichia coli (enterotoxigenic isolates), Campylobacter jejuni, Shigella boydii†, Shigella dysenteriae, Shigella flexneri or Shigella sonnei† when antibacterial therapy is indicated.
† Although treatment of infections due to this organism in this organ system demonstrated a clinically significant outcome, efficacy was studied in fewer than 10 patients.
1.5 Typhoid Fever (Enteric Fever)
CIPRO is indicated in adult patients for treatment of typhoid fever (enteric fever) caused by Salmonella typhi. The efficacy of ciprofloxacin in the eradication of the chronic typhoid carrier state has not been demonstrated.
1.6 Uncomplicated Cervical and Urethral Gonorrhea
CIPRO is indicated in adult patients for treatment of uncomplicated cervical and urethral gonorrhea due to Neisseria gonorrhoeae [see Warnings and Precautions (5.17)].
1.7 Inhalational Anthrax (Post-Exposure)
CIPRO is indicated in adults and pediatric patients from birth to 17 years of age for inhalational anthrax (post-exposure) to reduce the incidence or progression of disease following exposure to aerosolized Bacillus anthracis.
Ciprofloxacin serum concentrations achieved in humans served as a surrogate endpoint reasonably likely to predict clinical benefit and provided the initial basis for approval of this indication1. Supportive clinical information for ciprofloxacin for anthrax post-exposure prophylaxis was obtained during the anthrax bioterror attacks of October 2001 [see Clinical Studies (14.2)].
1.8 Plague
CIPRO is indicated for treatment of plague, including pneumonic and septicemic plague, due to Yersinia pestis (Y. pestis) and prophylaxis for plague in adults and pediatric patients from birth to 17 years of age. Efficacy studies of ciprofloxacin could not be conducted in humans with plague for feasibility reasons. Therefore this indication is based on an efficacy study conducted in animals only [see Clinical Studies (14.3)].
1.9 Chronic Bacterial Prostatitis
CIPRO is indicated in adult patients for treatment of chronic bacterial prostatitis caused by Escherichia coli or Proteus mirabilis.
1.10 Lower Respiratory Tract Infections
CIPRO is indicated in adult patients for treatment of lower respiratory tract infections caused by Escherichia coli, Klebsiella pneumoniae, Enterobacter cloacae, Proteus mirabilis, Pseudomonas aeruginosa, Haemophilus influenzae, Haemophilus parainfluenzae, or Streptococcus pneumoniae.
CIPRO is not a drug of first choice in the treatment of presumed or confirmed pneumonia secondary to Streptococcus pneumoniae.
CIPRO is indicated for the treatment of acute exacerbations of chronic bronchitis (AECB) caused by Moraxella catarrhalis.
Because fluoroquinolones, including CIPRO, have been associated with serious adverse reactions [see Warnings and Precautions (5.1–5.16)] and for some patients AECB is self-limiting, reserve CIPRO for treatment of AECB in patients who have no alternative treatment options.
1.11 Urinary Tract Infections
Urinary Tract Infections in Adults
CIPRO is indicated in adult patients for treatment of urinary tract infections caused by Escherichia coli, Klebsiella pneumoniae, Enterobacter cloacae, Serratia marcescens, Proteus mirabilis, Providencia rettgeri, Morganella morganii, Citrobacter koseri, Citrobacter freundii, Pseudomonas aeruginosa, methicillin-susceptible Staphylococcus epidermidis, Staphylococcus saprophyticus, or Enterococcus faecalis.
Acute Uncomplicated Cystitis
CIPRO is indicated in adult female patients for treatment of acute uncomplicated cystitis caused by Escherichia coli or Staphylococcus saprophyticus.
Because fluoroquinolones, including CIPRO, have been associated with serious adverse reactions [see Warnings and Precautions (5.1-5.16)] and for some patients acute uncomplicated cystitis is self-limiting, reserve CIPRO for treatment of acute uncomplicated cystitis in patients who have no alternative treatment options.
Complicated Urinary Tract Infection and Pyelonephritis in Pediatric Patients
CIPRO is indicated in pediatric patients aged one to 17 years of age for treatment of complicated urinary tract infections (cUTI) and pyelonephritis due to Escherichia coli [see Use in Specific Populations (8.4)].
Although effective in clinical trials, CIPRO is not a drug of first choice in the pediatric population due to an increased incidence of adverse reactions compared to controls, including reactions related to joints and/or surrounding tissues. CIPRO, like other fluoroquinolones, is associated with arthropathy and histopathological changes in weight-bearing joints of juvenile animals [see Warnings and Precautions (5.13), Adverse Reactions (6.1), Use in Specific Populations (8.4) and Nonclinical Toxicology (13.2)].
1.12 Acute Sinusitis
CIPRO is indicated in adult patients for treatment of acute sinusitis caused by Haemophilus influenzae, Streptococcus pneumoniae, or Moraxella catarrhalis.
Because fluoroquinolones, including CIPRO, have been associated with serious adverse reactions [see Warnings and Precautions (5.1-5.16)] and for some patients acute sinusitis is self-limiting, reserve CIPRO for treatment of acute sinusitis in patients who have no alternative treatment options.
1.13 Usage
To reduce the development of drug-resistant bacteria and maintain the effectiveness of CIPRO and other antibacterial drugs, CIPRO should be used only to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.
If anaerobic organisms are suspected of contributing to the infection, appropriate therapy should be administered. Appropriate culture and susceptibility tests should be performed before treatment in order to isolate and identify organisms causing infection and to determine their susceptibility to ciprofloxacin. Therapy with CIPRO may be initiated before results of these tests are known; once results become available appropriate therapy should be continued.
As with other drugs, some isolates of Pseudomonas aeruginosa may develop resistance fairly rapidly during treatment with ciprofloxacin. Culture and susceptibility testing performed periodically during therapy will provide information not only on the therapeutic effect of the antimicrobial agent but also on the possible emergence of bacterial resistance.
2. Dosage and Administration
CIPRO Tablets and Oral Suspension should be administered orally as described in the appropriate Dosage Guidelines tables.
2.1 Dosage in Adults
The determination of dosage and duration for any particular patient must take into consideration the severity and nature of the infection, the susceptibility of the causative microorganism, the integrity of the patient's host-defense mechanisms, and the status of renal and hepatic function. CIPRO Tablets or Oral Suspension may be administered to adult patients when clinically indicated at the discretion of the physician. Administer CIPRO for Oral Suspension using the co-packaged graduated spoon [see Dosage and Administration (2.7)].
Table 1. Adult Dosage Guidelines:
| Infection | Dose | Frequency | Usual Durations* |
|---|---|---|---|
| Skin and Skin Structure | 500–750 mg | every 12 hours | 7 to 14 days |
| Bone and Joint | 500–750 mg | every 12 hours | 4 to 8 weeks |
| Complicated Intra–Abdominal† | 500 mg | every 12 hours | 7 to 14 days |
| Infectious Diarrhea | 500 mg | every 12 hours | 5 to 7 days |
| Typhoid Fever | 500 mg | every 12 hours | 10 days |
| Uncomplicated Urethral and Cervical Gonococcal Infections | 250 mg | single dose | single dose |
| Inhalational anthrax (post-exposure)‡ | 500 mg | every 12 hours | 60 days |
| Plague‡ | 500–750 mg | every 12 hours | 14 days |
| Chronic Bacterial Prostatitis | 500 mg | every 12 hours | 28 days |
| Lower Respiratory Tract Infections | 500–750 mg | every 12 hours | 7 to 14 days |
| Urinary Tract Infections | 250–500 mg | every 12 hours | 7 to 14 days |
| Acute Uncomplicated Cystitis | 250 mg | every 12 hours | 3 days |
| Acute Sinusitis | 500 mg | every 12 hours | 10 days |
* Generally ciprofloxacin should be continued for at least 2 days after the signs and symptoms of infection have disappeared, except for inhalational anthrax (post-exposure).
† Used in conjunction with metronidazole.
‡ Begin drug administration as soon as possible after suspected or confirmed exposure.
Conversion of IV to Oral Dosing in Adults
Patients whose therapy is started with CIPRO IV may be switched to CIPRO Tablets or Oral Suspension when clinically indicated at the discretion of the physician (Table 2) [see Clinical Pharmacology (12.3)].
Table 2. Equivalent AUC Dosing Regimens:
| CIPRO Oral Dosage | Equivalent CIPRO IV Dosage |
|---|---|
| 250 mg Tablet every 12 hours | 200 mg intravenous every 12 hours |
| 500 mg Tablet every 12 hours | 400 mg intravenous every 12 hours |
| 750 mg Tablet every 12 hours | 400 mg intravenous every 8 hours |
2.2 Dosage in Pediatric Patients
Dosing and initial route of therapy (that is, IV or oral) for cUTI or pyelonephritis should be determined by the severity of the infection. CIPRO should be administered as described in Table 3. Administer CIPRO for Oral Suspension using the co-packaged graduated spoon [see Dosage and Administration (2.7)].
Table 3. Pediatric Dosage Guidelines:
| Infection | Dose | Frequency | Total Duration |
|---|---|---|---|
| Complicated Urinary Tract or Pyelonephritis (patients from 1 to 17 years of age) | 10 mg/kg to 20 mg/kg (maximum 750 mg per dose; not to be exceeded even in patients weighing more than 51 kg) | every 12 hours | 10–21 days |
| Inhalational Anthrax (Post-Exposure)2 | 15 mg/kg(maximum 500 mg per dose) | every 12 hours | 60 days |
| Plague2,3 | 15 mg/kg (maximum 500 mg per dose) | every 8 to 12 hours | 14 days |
2.3 Dosage Modifications in Patients with Renal Impairment
Ciprofloxacin is eliminated primarily by renal excretion; however, the drug is also metabolized and partially cleared through the biliary system of the liver and through the intestine. These alternative pathways of drug elimination appear to compensate for the reduced renal excretion in patients with renal impairment. Nonetheless, some modification of dosage is recommended, particularly for patients with severe renal dysfunction. Dosage guidelines for use in patients with renal impairment are shown in Table 4.
Table 4. Recommended Starting and Maintenance Doses for Adult Patients with Impaired Renal Function:
| Creatinine Clearance (mL/min) | Dose |
|---|---|
| >50 | See Usual Dosage. |
| 30–50 | 250–500 mg every 12 hours |
| 5–29 | 250–500 mg every 18 hours |
| Patients on hemodialysis or Peritoneal dialysis | 250–500 mg every 24 hours (after dialysis) |
When only the serum creatinine concentration is known, the following formulas may be used to estimate creatinine clearance:
Men - Creatinine clearance (mL/min) = Weight (kg) x (140–age) / 72 x serum creatinine (mg/dL)
Women - 0.85 x the value calculated for men.
The serum creatinine should represent a steady state of renal function.
In patients with severe infections and severe renal impairment, a unit dose of 750 mg may be administered at the intervals noted above. Patients should be carefully monitored.
Pediatric patients with moderate to severe renal insufficiency were excluded from the clinical trial of cUTI and pyelonephritis. No information is available on dosing adjustments necessary for pediatric patients with moderate to severe renal insufficiency (that is, creatinine clearance of <50 mL/min/1.73m²).
2.4 Important Administration Instructions
With Multivalent Cations
Administer CIPRO at least 2 hours before or 6 hours after magnesium/aluminum antacids; polymeric phosphate binders (for example, sevelamer, lanthanum carbonate) or sucralfate; Videx (didanosine) chewable/buffered tablets or pediatric powder for oral solution; other highly buffered drugs; or other products containing calcium, iron or zinc.
With Dairy Products
Concomitant administration of CIPRO with dairy products (like milk or yogurt) or calcium-fortified juices alone should be avoided since decreased absorption is possible; however, CIPRO may be taken with a meal that contains these products.
Hydration of Patients Receiving CIPRO
Assure adequate hydration of patients receiving CIPRO to prevent the formation of highly concentrated urine. Crystalluria has been reported with quinolones.
Instruct the patient of the appropriate CIPRO administration [see Patient Counseling Information (17)].
Missed Doses
If a dose is missed, it should be taken anytime but not later than 6 hours prior to the next scheduled dose. If less than 6 hours remain before the next dose, the missed dose should not be taken and treatment should be continued as prescribed with the next scheduled dose. Double doses should not be taken to compensate for a missed dose.
2.5 Directions for Reconstitution of the CIPRO Microcapsules for Oral Suspension
CIPRO Oral Suspension is supplied in 5% (5 g ciprofloxacin in 100 mL) and 10% (10 g ciprofloxacin in 100 mL) strengths. CIPRO oral suspension is composed of two components (microcapsules and diluent) that must be combined prior to dispensing.
Table 5. Appropriate Dosing Volumes of the Reconstituted Oral Suspensions:
| Dose | 5% (250 mg/5 mL) | 10% (500 mg/5 mL) |
|---|---|---|
| 250 mg | 5 mL | 2.5 mL |
| 500 mg | 10 mL | 5 mL |
| 750 mg | 15 mL | 7.5 mL |
Preparation of the suspension:
Step 1: The small bottle contains the microcapsules, the large bottle contains the diluent.
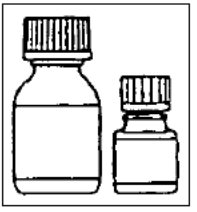
Step 2: Open both bottles. Child-proof cap: Press down according to instructions on the cap while turning to the left.

Step 3: Pour the microcapsules completely into the larger bottle of diluent. Do not add water to the suspension.

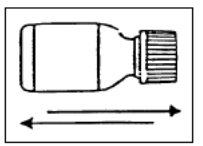
Step 4: Remove the top layer of the diluent bottle label (to reveal the CIPRO Oral Suspension label). Close the large bottle completely according to the directions on the cap and shake vigorously for about 15 seconds. The suspension is ready for use.
Step 5: Write the expiration date of the re-constituted oral suspension on the bottle label.
Reconstituted product may be stored below 30°C (86°F) for 14 days. Protect from freezing.
No additions should be made to the mixed final ciprofloxacin suspension. CIPRO Oral Suspension should not be administered through feeding or NG (nasogastric) tubes due to its physical characteristics.
2.6 Administration Instructions for CIPRO for Oral Suspension After Reconstitution
- Shake CIPRO Oral Suspension vigorously each time before use for approximately 15 seconds.
- Administer CIPRO Oral Suspension using the co-packaged graduated teaspoon provided for the patient (see Figure 1)
Figure 1. Co-packaged 5 mL graduated teaspoon:
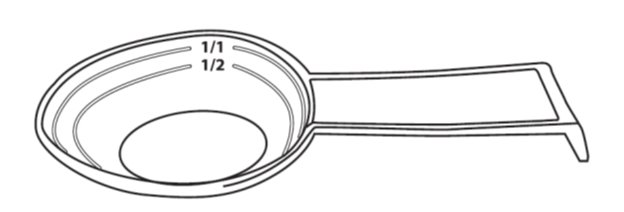
The Co-packaged graduated teaspoon (5mL) is provided, with markings for ½ (2.5 mL) and 1/1 (5 mL).
- After use, clean the graduated teaspoon under running water with dish detergent and dry thoroughly.
- Do Not chew the microcapsules in the CIPRO Oral Suspension, instead swallow them whole.
- Water may be taken afterwards.
- Reclose the bottle properly after each use according to instructions on the cap.
After treatment has been completed, CIPRO Oral Suspension should not be reused.
2.7 Dosing of CIPRO for Oral Suspension using the Co-Packaged Spoon in Adults and Pediatric Patients
Table. 5% Cipro for Oral Suspension: 250 mg ciprofloxacin per 5 mL after reconstitution:
| Infection | Body weight (kg) | Dose by Measuring Spoonful(s) using Co-Packed Spoon* (teaspoonful (s) (volume (mL)) | Dose Strength (mg) |
|---|---|---|---|
| Complicated Urinary Tract or Pyelonephritis (patients from 1 to 17 years of age)1 and Plague2 | 9 kg to 12 kg | ½ teaspoonful (2.5 mL) | 125 mg |
| 13 kg to 18 kg | 1 teaspoonful (5 mL) | 250 mg | |
| 19 kg to 24 kg | 1 to 1 ½ teaspoonful(s) (5 mL to 7.5 mL) | 250 mg to 375 mg | |
| 25 kg to 31 kg | 1 ½ to 2 teaspoonfuls (7.5 mL to 10 mL) | 375 mg to 500 mg | |
| 32 kg to 37 kg | 1 ½ to 2 ½ teaspoonfuls (7.5 mL to 12.5 mL) | 375 mg to 625 mg | |
| 38 kg or more | 2 to 3 teaspoonfuls (10 mL to 15 mL) | 500 mg to 750 mg | |
| Inhalational Anthrax (Post-Exposure) 3 | 9 kg to 12 kg | ½ teaspoonful (2.5 mL) | 125 mg |
| 13 kg to 18 kg | 1 teaspoonful (5 mL) | 250 mg | |
| 19 kg to 24 kg | 1 to 1 ½ teaspoonful(s) (5 mL to 7.5 mL) | 250 mg to 375 mg | |
| 25 kg or more | 2 teaspoonfuls (10 mL) | 500 mg |
* A graduated teaspoon (5mL) with markings ½ (2.5) mL and 1/1 (5 mL) is provided for the patient.
1 Administer every 12 hours for 10-21 days [see Dosage and Administration (2.2)]
2 Administer every 8-12 hours for 10-21 days for Pediatric patients [see Dosage and Administration (2.2)]; for adults administer every 12 hours for 14 days [see Dosage and Administration (2.1)]
3 Administer every 12 hours for 60 days [see Dosage and Administration (2.1 and 2.2)]
Table 7. 10% Oral Suspension: 500 mg ciprofloxacin per 5 mL after reconstitution (not appropriate for children weighing less than 13 kg):
| Infection | Body weight (kg) | Dose by Measuring Spoonful(s) using Co-Packed Spoon* (teaspoonful (s) (volume (mL)) | Dose Strength (mg) |
|---|---|---|---|
| Complicated Urinary Tract or Pyelonephritis (patients from 1 to 17 years of age)1 and Plague2 | 13 kg to 24 kg | ½ teaspoonful (2.5 mL) | 250 mg |
| 25 kg | ½ to 1 teaspoonful (2.5 mL to 5 mL) | 250 mg to 500 mg | |
| 26 kg to 37 kg | 1 teaspoonful (5 mL) | 500 mg | |
| 38 kg or more | 1 to 1½ teaspoonful(s) (5 mL to 7.5 mL) | 500 mg to maximum dose of 750 mg | |
| Inhalational Anthrax (Post-Exposure)3 | 13 kg to 24 kg | ½ teaspoonful (2.5 mL) | 250 mg |
| 25 kg or more | 1 teaspoonful (5 mL) | 500 mg |
* A graduated teaspoon (5mL) with markings ½ (2.5) mL and 1/1 (5 mL) is provided for the patient.
1 Administer every 12 hours for 10-21 days [see Dosage and Administration (2.2)]
2 Administer every 8-12 hours for 10-21 days for Pediatric patients [see Dosage and Administration (2.2)]; for adults administer every 12 hours for 14 days [see Dosage and Administration (2.1)]
3 Administer every 12 hours for 60 days [see Dosage and Administration (2.1 and 2.2)]
10. Overdosage
In the event of acute overdosage, reversible renal toxicity has been reported in some cases. Empty the stomach by inducing vomiting or by gastric lavage. Observe the patient carefully and give supportive treatment, including monitoring of renal function, urinary pH and acidify, if required, to prevent crystalluria and administration of magnesium, aluminum, or calcium containing antacids which can reduce the absorption of ciprofloxacin. Adequate hydration must be maintained. Only a small amount of ciprofloxacin (less than 10%) is removed from the body after hemodialysis or peritoneal dialysis.
16.2. Storage and Handling
CIPRO (ciprofloxacin hydrochloride) Tablets:
Store at 20° to 25°C (68° to 77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature].
CIPRO Oral Suspension:
Store microcapsules and diluent below 25°C (77°F); excursions are permitted from 15°C to 30°C (59°F to 86°F) [see USP Controlled Room Temperature]. Protect from freezing.
The reconstituted product may be stored at 25°C (77°F) for 14 days; excursions are permitted from 15°C to 30°C (59°F to 86°F) [see USP Controlled Room Temperature]. Protect from freezing.
A graduated teaspoon (5mL) with markings ½ (2.5 mL) and 1/1 (5 mL) is provided for the patient.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.