Source: European Medicines Agency (EU) Revision Year: 2023 Publisher: Vertex Pharmaceuticals (Ireland) Limited, Unit 49, Block F2, Northwood Court, Santry, Dublin 9, D09 T665, Ireland
Pharmacotherapeutic group: Other respiratory system products
ATC code: R07AX30
The CFTR protein is a chloride channel present at the surface of epithelial cells in multiple organs. The F508del mutation impacts the CFTR protein in multiple ways, primarily by causing a defect in cellular processing and trafficking that reduces the quantity of CFTR at the cell surface. The small amount of F508del-CFTR that reaches the cell surface has low channel-open probability (defective channel gating). Lumacaftor is a CFTR corrector that acts directly on F508del-CFTR to improve its cellular processing and trafficking, thereby increasing the quantity of functional CFTR at the cell surface. Ivacaftor is a CFTR potentiator that facilitates increased chloride transport by potentiating the channel-open probability (or gating) of the CFTR protein at the cell surface. The combined effect of lumacaftor and ivacaftor is increased quantity and function of F508delCFTR at the cell surface, resulting in increased chloride ion transport. The exact mechanisms by which lumacaftor improves cellular processing and trafficking of F508delCFTR and ivacaftor potentiates F508del-CFTR are not known.
Changes in sweat chloride in response to lumacaftor alone or in combination with ivacaftor were evaluated in a double-blind, placebo-controlled, Phase 2 clinical trial in patients with CF aged 18 years and older. In this trial, 10 patients (homozygous for F508del-CFTR mutation) completed dosing with lumacaftor alone 400 mg q12h for 28 days followed by the addition of ivacaftor 250 mg q12h for an additional 28 days, and 25 patients (homozygous or heterozygous for F508del) completed dosing with placebo. The treatment difference between lumacaftor 400 mg q12h alone and placebo evaluated as mean change in sweat chloride from baseline to day 28 was statistically significant at -8.2 mmol/L (95% CI: -14, -2). The treatment difference between the combination of lumacaftor 400 mg/ivacaftor 250 mg q12h and placebo evaluated as mean change in sweat chloride from baseline to day 56 was statistically significant at -11 mmol/L (95% CI: -18, -4).
In trial 809-109 (see Clinical efficacy and safety) in patients homozygous for the F508del-CFTR mutation aged 6 to less than 12 years, the treatment difference (LS mean) in sweat chloride for the absolute change at week 24 as compared to placebo was -24.9 mmol/L (nominal P<0.0001). The treatment difference (LS mean) in sweat chloride for the average absolute change at day 15 and at week 4 as compared to placebo was -20.8 mmol/L (95% CI: -23.4, -18.2; nominal P<0.0001).
In trial 809-115 in patients homozygous for F508del-CFTR mutation aged 2 to 5 years, the mean absolute within-group change in sweat chloride from baseline at week 24 was -31.7 mmol/L (95% CI: -35.7, -27.6). In addition, the mean absolute change in sweat chloride from week 24 at week 26 following the 2-week washout period (to evaluate off-drug response) was an increase of 33.0 mmol/L (95% CI: 28.9, 37.1; nominal P<0.0001), representing a return to baseline after treatment washout. At week 24, 16% of children had a reduction in sweat chloride below 60 mmol/L, and none below 30 mmol/L.
In trial 809-122 in patients homozygous for F508del-CFTR mutation aged 1 to less than 2 years, treatment with lumacaftor/ivacaftor demonstrated a reduction in sweat chloride at week 4 which was sustained through week 24. The mean absolute change from baseline in sweat chloride at week 24 was -29.1(13.5) mmol/L (95% CI: -34.8, -23.4). In addition, the mean (SD) absolute change in sweat chloride from week 24 at week 26 following the 2-week washout period was 27.3 (11.1) mmol/L (95% CI: 22.3, 32.3). This change represents a return towards baseline after treatment washout.
Changes in ppFEV1 in response to lumacaftor alone or in combination with ivacaftor were also evaluated in the double-blind, placebo-controlled, Phase 2 trial in patients with CF aged 18 years and older. The treatment difference between lumacaftor 400 mg q12h alone and placebo evaluated as mean absolute change in ppFEV1 was -4.6 percentage points (95% CI: -9.6, 0.4) from baseline to day 28, 4.2 percentage points (95% CI: –1.3, 9.7) from baseline to day 56, and 7.7 percentage points (95% CI: 2.6, 12.8; statistically significant) from day 28 to day 56 (following the addition of ivacaftor to lumacaftor monotherapy).
During the 24-week, placebo-controlled, Phase 3 studies, a maximum decrease in mean heart rate of 6 beats per minute (bpm) from baseline was observed on day 1 and day 15 around 4 to 6 hours after dosing. After day 15, heart rate was not monitored in the period after dosing in these studies. From week 4, the change in mean heart rate at pre-dose ranged from 1 to 2 bpm below baseline among patients treated with lumacaftor/ivacaftor. The percentage of patients with heart rate values <50 bpm on treatment was 11% for patients who received lumacaftor/ivacaftor, compared to 4.9% for patients who received placebo.
No meaningful changes in QTc interval or blood pressure were observed in a thorough QT clinical study evaluating lumacaftor 600 mg once daily/ivacaftor 250 mg q12h and lumacaftor 1000 mg once daily/ivacaftor 450 mg q12h.
The efficacy of lumacaftor/ivacaftor in patients with CF who are homozygous for the F508del mutation in the CFTR gene was evaluated in two randomised, double-blind, placebo-controlled clinical trials of 1.108 clinically stable patients with CF, in which 737 patients were randomised to and dosed with lumacaftor/ivacaftor. Patients in both trials were randomised 1:1:1 to receive lumacaftor 600 mg once daily/ivacaftor 250 mg q12h, lumacaftor 400 mg q12h/ivacaftor 250 mg q12h, or placebo. Patients took the study drug with fat-containing food for 24 weeks in addition to their prescribed CF therapies (e.g., bronchodilators, inhaled antibiotics, dornase alfa, and hypertonic saline). Patients from these trials were eligible to roll over into a blinded extension study.
Trial 809-103 evaluated 549 patients with CF who were aged 12 years and older (mean age 25.1 years) with percent predicted FEV1 (ppFEV1) at screening between 40-90 (mean ppFEV1 60.7 at baseline [range: 31.1 to 94.0]). Trial 809-104 evaluated 559 patients aged 12 years and older (mean age 25.0 years) with ppFEV1 at screening between 40-90 (mean ppFEV1 60.5 at baseline [range: 31.3 to 99.8]). Patients with a history of colonisation with organisms such as Burkholderia cenocepacia, Burkholderia dolosa, or Mycobacterium abscessus or who had 3 or more abnormal liver function tests (ALT, AST, AP, GGT ≥3 times the ULN or total bilirubin ≥2 times the ULN) were excluded.
The primary efficacy endpoint in both studies was the absolute change from baseline in ppFEV1 at week 24. Other efficacy variables included relative change from baseline in ppFEV1, absolute change from baseline in BMI, absolute change from baseline in CFQ-R Respiratory Domain, the proportion of patients achieving ≥5% relative change from baseline in ppFEV1 at week 24, and the number of pulmonary exacerbations (including those requiring hospitalisation or IV antibiotic therapy) through week 24.
In both trials, treatment with lumacaftor/ivacaftor resulted in a statistically significant improvement in ppFEV1 (see Table 6). Mean improvement in ppFEV1 was rapid in onset (day 15) and sustained throughout the 24-week treatment period. At day 15, the treatment difference between lumacaftor 400 mg/ivacaftor 250 mg q12h and placebo for the mean absolute change (95% CI) in ppFEV1 from baseline was 2.51 percentage points in the pooled trials 809-103 and 809-104 (P<0.0001). Improvements in ppFEV1 were observed regardless of age, disease severity, sex and geographic region. The Phase 3 trials of lumacaftor/ivacaftor included 81 patients with ppFEV1 <40 at baseline. The treatment difference in this subgroup was comparable to that observed in patients with ppFEV1 ≥40. At week 24, the treatment difference between lumacaftor 400 mg/ivacaftor 250 mg q12h and placebo for the mean absolute change (95% CI) in ppFEV1 from baseline in the pooled trials 809-103 and 809-104 were 3.39 percentage points (P=0.0382) for patients with ppFEV1 <40 and 2.47 percentage points (P<0.0001) for patients with ppFEV1 ≥40.
Table 6. Summary of primary and key secondary outcomes in trial 809-103 and trial 809-104*:
| Trial 809-103 | Trial 809-104 | Pooled (trial 809-103 and 809-104) | |||||
|---|---|---|---|---|---|---|---|
| Placebo (n=184) | LUM 400 mg q12h/IVA 250 mg q12h (n=182) | Placebo (n=187) | LUM 400 mg q12h/IVA 250 mg q12h (n=187) | Placebo (n=371) | LUM 400 mg q12h/IVA 250 mg q12h (n=369) | ||
| Absolute change in ppFEV1 at week 24 (percentage points)) | Treatment difference | – | 2.41 (P=0.0003)† | – | 2.65 (P=0.0011)† | – | 2.55 (P<0.0001) |
| Within-group change | -0.73 (P=0.2168) | 1.68 (P=0.0051) | -0.02 (P=0.9730) | 2.63 (P<0.0001) | -0.39 (P<0.3494) | 2.16 (P<0.0001) | |
| Relative change in ppFEV1 at week 24 (%) | Treatment difference | – | 4.15 (P=0.0028)† | – | 4.69 (P=0.0009)† | – | 4.4 (P<0.0001) |
| Within-group change | -0.85 (P=0.3934) | 3.3 (P=0.0011) | 0.16 (P=0.8793) | 4.85 (P<0.0001) | -0.34 (P=0.6375) | 4.1 (P<0.0001) | |
| Absolute change in BMI at week 24 (kg/m²) | Treatment difference | – | 0.13 (P=0.1938) | – | 0.36 (P<0.0001)† | – | 0.24 (P=0.0004) |
| Within-group change | 0.19 (P=0.0065) | 0.32 (P<0.0001) | 0.07 (P=0.2892) | 0.43 (P<0.0001) | 0.13 (P=0.0066) | 0.37 (P<0.0001) | |
| Absolute change in CFQ-R Respiratory Domain Score at week 24 (points) | Treatment difference | – | 1.5 (P=0.3569) | – | 2.9 (P=0.0736) | – | 2.2 (P=0.0512) |
| Within-group change | 1.1 (P=0.3423) | 2.6 (P=0.0295) | 2.8 (P=0.0152) | 5.7 (P<0.0001) | 1.9 (P=0.0213) | 4.1 (P<0.0001) | |
| Proportion of patients with ≥5% relative change in ppFEV1 at week 24 | % | 25% | 32% | 26% | 41% | 26% | 37% |
| Odds ratio | – | 1.43 (P=0.1208) | – | 1.90 (P=0.0032) | – | 1.66 (P=0.0013) | |
| Number of pulmonary exacerbations through week 24 | # of events (rate per 48 weeks) | 112 (1.07) | 73 (0.71) | 139 (1.18) | 79 (0.67) | 251 (1.14) | 152 (0.70) |
| Rate ratio | – | 0.66 (P=0.0169) | – | 0.57 (P=0.0002) | – | 0.61 (P<0.0001) | |
In each study, a hierarchical testing procedure was performed within each active treatment arm for primary and secondary endpoints vs. placebo; at each step, P≤0.0250 and all previous tests also meeting this level of significance was required for statistical significance.
† Indicates statistical significance confirmed in the hierarchical testing procedure.
At week 24, the proportion of patients who remained free from pulmonary exacerbations was significantly higher for patients treated with lumacaftor/ivacaftor compared with placebo. In the pooled analysis, the rate ratio of exacerbations through week 24 in subjects treated with lumacaftor/ivacaftor (lumacaftor 400 mg/ivacaftor 250 mg q12h; n=369) was 0.61 (P<0.0001), representing a reduction of 39% relative to placebo. The event rate per year, annualised to 48 weeks, was 0.70 in the lumacaftor/ivacaftor group and 1.14 in the placebo group. Treatment with lumacaftor/ivacaftor significantly decreased the risk for exacerbations requiring hospitalisation versus placebo by 61% (rate ratio=0.39, P<0.0001; event rate per 48 weeks 0.17 for lumacaftor/ivacaftor and 0.45 for placebo) and reduced exacerbations requiring treatment with intravenous antibiotics by 56% (rate ratio = 0.44, P<0.0001; event rate per 48 weeks 0.25 for lumacaftor/ivacaftor and 0.58 for placebo). These results were not considered statistically significant within the framework of the testing hierarchy for the individual studies.
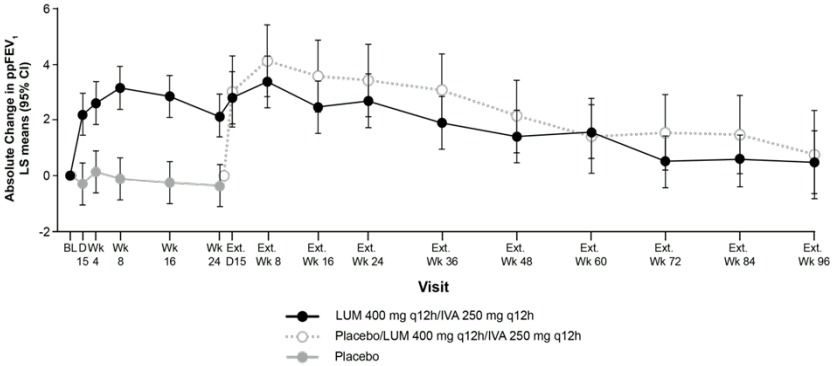
Trial 809-105 was a Phase 3, parallel-group, multicentre, rollover extension study in patients with CF that included patients aged 12 years and older from trial 809-103 and trial 809-104. This extension trial was designed to evaluate the safety and efficacy of long-term treatment of lumacaftor/ivacaftor. Of the 1.108 patients who received any treatment in trial 809-103 or trial 809-104, 1.029 (93%) were dosed and received active treatment (lumacaftor 600 mg once daily/ivacaftor 250 mg q12h or lumacaftor 400 mg q12h/ivacaftor 250 mg q12h) in trial 809-105 for up to an additional 96 weeks (i.e., up to a total of 120 weeks). The primary efficacy analysis of this extension study included data up to week 72 of trial 809-105 with a sensitivity analysis that included data up to week 96 of trial 809-105. Patients treated with lumacaftor/ivacaftor in trial 809-103 or trial 809-104 showed an effect that was maintained with respect to baseline after an additional 96 weeks through trial 809-105. For patients who transitioned from placebo to active treatment similar changes as those observed in patients treated with lumacaftor/ivacaftor in trial 809-103 or trial 809-104 were seen (see Table 6). Results from trial 809-105 are presented in Figure 1 and Table 7.
Figure 1. Absolute change from baseline in percent predicted FEV1 at each visit†:
† From trials 809-103, 809-104 and 809-105.
Table 7. Long-term effect of lumacaftor/ivacaftor in trial 809-105*:
| Baseline and endpoint | Placebo transitioned to lumacaftor 400 mg q12h/ ivacaftor 250 mg q12h (n=176)** | lumacaftor 400 mg q12h/ ivacaftor 250 mg q12h (n=369)† | ||||
|---|---|---|---|---|---|---|
| Mean (SD) | LS Means (95% CI) | τιμή P | Mean (SD) | LS Means (95% CI) | τιμή P | |
| Baseline ppFEV1‡ | 60.2 (14.7) | 60.5 (14.1) | ||||
| Absolute change from baseline ppFEV1 (percentage points) | ||||||
| Extension week 72 | (n=134) 1.5 (0.2, 2.9) | 0.0254 | (n=273) 0.5 (-0.4, 1.5) | 0.2806 | ||
| Extension week 96 | (n=75) 0.8 (-0.8, 2.3) | 0.3495 | (n=147) 0.5 (-0.7, 1.6) | 0.4231 | ||
| Relative change from baseline ppFEV1 (%) | ||||||
| Extension week 72 | (n=134) 2.6 (0.2, 5.0) | 0.0332 | (n=273) 1.4 (-0.3, 3.2) | 0.1074 | ||
| Extension week 96 | (n=75) 1.1 (-1.7, 3.9) | 0.4415 | (n=147) 1.2 (-0.8, 3.3) | 0.2372 | ||
| Baseline BMI (kg/m²)‡ | 20.9 (2.8) | 21.5 (3.0) | ||||
| Absolute change from baseline in BMI (kg/m²) | ||||||
| Extension week 72 | 0.62 (0.45, 0.79) | <0.0001 | (n=289) 0.69 (0.56, 0.81) | <0.0001 | ||
| Extension week 96 | (n=80) 0.76 (0.56, 0.97) | <0.0001 | (n=155) 0.96 (0.81, 1.11) | <0.0001 | ||
| Baseline CFQ-R Respiratory Domain Score (points)‡ | 70.4 (18.5) | 68.3 (18.0) | ||||
| Absolute change in CFQ-R Respiratory Domain Score (points) | ||||||
| Extension week 72 | 3.3 (0.7, 5.9) | 0.0124 | (n=269) 5.7 (3.8, 7.5) | <0.0001 | ||
| Extension week 96 | 0.5 (-2.7, 3.6) | 0.7665 | (n=165) 3.5 (1.3, 5.8) | 0.0018 | ||
| Number of Pulmonary exacerbations**,†,*** (events) | ||||||
| Number of events per patient-year (95% CI) (rate per 48 weeks) | 0.69 (0.56, 0.85) | 0.65 (0.56, 0.75) | ||||
| Number of events requiring hospitalization per patient-year (95% CI) (rate per 48 weeks) | 0.30 (0.22, 0.40) | 0.24 (0.19, 0.29) | ||||
| Number of events requiring intravenous antibiotics per patient- year (95% CI) (rate per 48 weeks) | 0.37 (0.29, 0.49) | 0.32 (0.26, 0.38) | ||||
* A total of 82% (421 of 516 eligible patients) completed 72 weeks of this study; 42% completed 96 weeks. Majority of patients discontinued for reasons other than safety.
** For patients rolled over from trials 809-103 and 809-104 (placebo-to-lumacaftor/ivacaftor group) total exposure was up to 96 weeks. Presentation of the lumacaftor 400 mg q12h/ivacaftor 250 mg q12h dose group is consistent with recommended posology.
*** The event rate per patient-year was annualised to 48 weeks.
† For patients rolled over from trials 809-103 and 809-104 (lumacaftor/ivacaftor-to-lumacaftor/ivacaftor group) total exposure was up to 120 weeks. Presentation of the lumacaftor 400 mg q12h/ivacaftor 250 mg q12h dose grou is consistent with recommended posology.
‡ Baseline for the placebo transitioned to lumacaftor 400 mg q12h/ivacaftor 250 mg q12h group was the trial 809-105 baseline. Baseline for the lumacaftor 400 mg q12h/ivacaftor 250 mg q12h group was the trial 809-103 and 809-104 baseline.
Trial 809-102 was a multicentre, double–blind, randomised, placebo–controlled, Phase 2 trial in 125 patients with CF aged 18 years and older who had a ppFEV1 of 40 to 90. inclusive, and have the F508del mutation on one allele plus a second allele with a mutation predicted to result in the lack of CFTR production or a CFTR that is not responsive to ivacaftor in vitro.
Patients received either lumacaftor/ivacaftor (n=62) or placebo (n=63) in addition to their prescribed CF therapies. The primary endpoint was improvement in lung function as determined by the mean absolute change from baseline at day 56 in ppFEV1. Treatment with lumacaftor/ivacaftor resulted in no significant improvement in ppFEV1 relative to placebo in patients with CF heterozygous for the F508del mutation in the CFTR gene (treatment difference 0.60 [P=0.5978]) and no meaningful improvements in BMI or weight (see section 4.4).
Trial 809-109 was a 24-week, placebo-controlled, Phase 3 clinical study in 204 patients with CF aged 6 to less than 12 years old (mean age 8.8 years). Trial 809-109 evaluated subjects with lung clearance index (LCI2.5) ≥7.5 at the initial screening visit (mean LCI2.5 10.28 at baseline [range: 6.55 to 16.38]) and ppFEV1 ≥70 at screening (mean ppFEV1 89.8 at baseline [range: 48.6 to 119.6]). Patients received either lumacaftor 200 mg/ivacaftor 250 mg every 12 hours (n=103) or placebo (n=101) in addition to their prescribed CF therapies. Patients who had 2 or more abnormal liver function tests (ALT, AST, AP, GGT ≥3 times the ULN), or ALT or AST >5 times ULN, or total bilirubin >2 times ULN were excluded.
The primary efficacy endpoint was absolute change in LCI2.5 from baseline through week 24. Key secondary endpoints included average absolute change from baseline in sweat chloride at day 15 and week 4 and at week 24 (see Pharmacodynamic effects), absolute change from baseline in BMI at week 24, absolute change from baseline in CFQ-R Respiratory Domain through week 24. These results are presented in Table 8 below:
Table 8. Summary of primary and key secondary outcomes in trial 809-109:
| Placebo (n=101) | LUM 200 mg/IVA 250 mg q12h (n=103) | ||
|---|---|---|---|
| Primary endpoint | |||
| Absolute change in lung clearance index (LCI2.5) from baseline through week 24 | Treatment difference | – | -1.09 (P<0.0001) |
| Within-group change | 0.08 (P=0.5390) | -1.01 (P<0.0001) | |
| Key Secondary Endpoints* | |||
| Absolute change in BMI at week 24 (kg/m²) | Treatment difference | – | 0.11 (P=0.2522) |
| Within-group change | 0.27 (P=0.0002) | 0.38 (P<0.0001) | |
| Absolute change in CFQ-R Respiratory Domain Score through week 24 (points) | Treatment difference | – | 2.5 (P=0.0628) |
| Within-group change | 3.0 (P=0.0035) | 5.5 (P<0.0001) | |
* Trial included key secondary and other secondary endpoints.
Percent predicted FEV1 was also evaluated as a clinically meaningful other secondary endpoint. In the lumacaftor/ivacaftor patients, the treatment difference for absolute change in ppFEV1 from baseline through week 24 was 2.4 (P=0.0182).
Patients with CF aged 6 years and older from trial 809-011 and trial 809-109 were included in a phase 3, multicentre, rollover extension study (trial -809-110). This extension trial was designed to evaluate the safety and efficacy of long-term treatment of lumacaftor/ivacaftor. Of the 262 patients who received any treatment in trial 809-011 or trial 809-109, 239 (91%) were dosed and received active treatment (patients 6 to <12 years of age received lumacaftor 200 mg q12h/ivacaftor 250 mg q12h; patients ≥12 years of age received lumacaftor 400 mg q12h/ivacaftor 250 mg q12h) in the extension study for up to an additional 96 weeks (i.e., up to a total of 120 weeks) (see section 4.8). Secondary efficacy results and pulmonary exacerbation event rate per patient year are presented in Table 9.
Table 9. Long-term effect of lumacaftor/ivacaftor in trial 809-110:
| Baseline and endpoint | Placebo transitioned to lumacaftor/ivacaftor (P-L/I) (n=96)* | lumacaftor/ivacaftor – lumacaftor/ivacaftor (L/I-L/I) (n=143)* | ||
|---|---|---|---|---|
| Mean (SD) | LS Mean (95% CI) | Mean (SD) | LS Mean (95% CI) | |
| n=101 | n=128 | |||
| Baseline LCI2.5‡** | 10.26 (2.24) | 10.24 (2.42) | ||
| Absolute change from baseline in LCI2.5 | ||||
| Extension week 96 | (n=69) -0.86 (-1.33, -0.38) | (n=88) -0.85 (-1.25, -0.45) | ||
| n=101 | n=161 | |||
| Baseline BMI (kg/m²)‡ | 16.55 (1.96) | 16.56 (1.77) | ||
| Absolute change from baseline in BMI (kg/m²) | ||||
| Extension week 96 | (n=83) 2.04 (1.77, 2.31) | (n=130) 1.78 (1.56, 1.99) | ||
| n=78 | n=135 | |||
| Baseline CFQ-R‡ Respiratory Domain Score (points) | 77.1 (15.5) | 78.5 (14.3) | ||
| Absolute change in CFQ-R Respiratory Domain Score (points) | ||||
| Extension week 96 | (n=65) 6.6 (3.1, 10.0) | (n=108) 7.4 (4.8, 10.0) | ||
| Number of pulmonary exacerbations (events) (trial 809-109 FAS and ROS)† | ||||
| Number of events per patient-year (95% CI) | n=96 0.30 (0.21, 0.43) | n=103 0.45 (0.33, 0.61) | ||
* Subjects treated with placebo in trial 809-109 (n=96) and transitioned onto active LUM/IVA treatment in the extension study (P-L/I). Subjects treated with LUM/IVA in either parent study [trial 809-011 (n=49) or trial 809-109 (n=94)] and continued active LUM/IVA treatment in the extension (L/I-L/I).
‡ Baseline for both groups (P-L/I and L/I-L/I) was the trial 809-011 and trial 809-109 (parent study) baseline and the corresponding n refers to the analysis set in the parent study.
** The LCI sub-study included 117 subjects in the L/I-L/I group and 96 subjects in the P-L/I group.
† FAS = Full Analysis Set (n=103) includes subjects who received L/I in trial 809-109 and in trial 809-110, assessed over the cumulative study period for L/I; ROS = Rollover Set (n=96) includes subjects who received placebo in trial 809-109 and L/I in trial 809-110, assessed over the current study period for trial 809-110.
Trial 809-115 evaluated 60 patients aged 2 to 5 years at screening (mean age at baseline 3.7 years). According to their weight at screening, patients were administered granules mixed with food every 12 hours, at a dose of lumacaftor 100 mg/ivacaftor 125 mg granules for patients weighing less than14 kg (n=19) or lumacaftor 150 mg/ivacaftor 188 mg for patients weighing 14 kg or greater (n=41), for 24 weeks in addition to their prescribed CF therapies. In order to evaluate off drug effects, patients had a safety follow-up visit following a 2-week washout period.
Secondary endpoints included absolute change from baseline in sweat chloride at week 24 and absolute change in sweat chloride from week 24 at week 26 (see Pharmacodynamic effects) as well as the endpoints listed in Table 10. The clinical relevance of the magnitude of these changes in children aged 2 to 5 years with cystic fibrosis has not been clearly ascertained in longer-term treatment.
Table 10. Summary of secondary outcomes in Trial 809-115:
| Secondary endpoints* | LUM/IVA |
|---|---|
| Absolute change from baseline in body mass index (BMI) | n=57 0.27 95% CI: 0.07, 0.47; P=0.0091 |
| Absolute change from baseline in BMI-for-age-z-score | n=57 0.29 95% CI: 0.14, 0.45; P=0.0003 |
| Absolute change from baseline in weight (kg) | n=57 1.4 95% CI: 1.2, 1.7; P<0.0001 |
| Absolute change from baseline in weight-for-age z-score | n=57 0.26 95% CI: 0.15, 0.38; P<0.0001 |
| Absolute change from baseline in stature (cm) | n=57 3.6 95% CI: 3.3, 3.9; P<0.0001 |
| Absolute change from baseline in stature-for-age z-score | n=57 0.09 95% CI: 0.02, 0.15; P=0.0104 |
| Absolute change from baseline in faecal elastase-1 (FE-1) levels (µg/g)** | n=35 52.6 95% CI: 22.5, 82.7; P=0.0012 |
| LCI2.5 | n=17 -0.58 95% CI: -1.17, 0.02; P=0.0559 |
Note: P values in the table are nominal.
* For the endpoints listed, absolute change from baseline is the mean absolute change from baseline at week 24.
** All patients had pancreatic insufficiency at baseline. Three of the 48 patients who had faecal elastase-1 values <100 µg/g at baseline achieved a level of ≥200 µg/g at week 24.
In Trial 809-122 Part B the primary endpoint of safety and tolerability was evaluated in 46 patients across 24 weeks (mean age at baseline 18.1 months). Secondary endpoints evaluated were pharmacokinetics and absolute change from baseline in sweat chloride at week 24 (see Pharmacodynamic effects). According to their weight at screening, patients were administered granules mixed with food every 12 hours for 24 weeks, at a dose of lumacaftor 75 mg/ivacaftor 94 mg granules (patients weighing 7 kg to <9 kg) or lumacaftor 100 mg/ivacaftor 125 mg granules (patients weighing 9 kg to <14 kg) or 150 mg lumacaftor/188 mg ivacaftor granules (patients weighing ≥14 kg), in addition to their prescribed CF therapies. In order to evaluate off-drug effects, patients had a safety follow-up visit following a 2-week washout period.
The European Medicines Agency has deferred the obligation to submit the results of studies with Orkambi in one or more subsets of the paediatric population in cystic fibrosis (see section 4.2 for information on paediatric use).
The exposure (AUC) of lumacaftor is approximately 2-fold higher in healthy adult volunteers compared to exposure in patients with CF. The exposure of ivacaftor is similar between healthy adult volunteers and patients with CF. After twice-daily dosing, steady-state plasma concentrations of lumacaftor and ivacaftor in healthy subjects were generally reached after approximately 7 days of treatment, with an accumulation ratio of approximately 1.9 for lumacaftor. The steady-state exposure of ivacaftor is lower than that of day 1 due to the CYP3A induction effect of lumacaftor (see section 4.5).
After oral administration of lumacaftor 400 mg q12h/ivacaftor 250 mg q12h in a fed state, the steady-state mean (± SD) for AUC0-12h and Cmax were 198 (64.8) µg∙h/mL and 25.0 (7.96) µg/mL for lumacaftor, respectively, and 3.66 (2.25) µg∙h/mL and 0.602 (0.304) µg/mL for ivacaftor, respectively. After oral administration of ivacaftor alone as 150 mg q12h in a fed state, the steady-state mean (± SD) for AUC0-12h and Cmax were 9.08 (3.20) µg∙h/mL and 1.12 (0.319) µg/mL, respectively.
Following multiple oral doses of lumacaftor, the exposure of lumacaftor generally increased proportional to dose over the range of 50 mg to 1000 mg every 24 hours. The exposure of lumacaftor increased approximately 2.0-fold when given with fat-containing food relative to fasted conditions. The median (range) Tmax of lumacaftor is approximately 4.0 hours (2.0; 9.0) in the fed state. Following multiple oral dose administration of ivacaftor in combination with lumacaftor, the exposure of ivacaftor generally increased with dose from 150 mg every 12 hours to 250 mg every 12 hours. The exposure of ivacaftor when given in combination with lumacaftor increased approximately 3-fold when given with fat-containing food in healthy volunteers. Therefore, lumacaftor/ivacaftor should be administered with fat-containing food. The median (range) Tmax of ivacaftor is approximately 4.0 hours (2.0; 6.0) in the fed state.
Lumacaftor is approximately 99% bound to plasma proteins, primarily to albumin. After oral administration of 400 mg every 12 hours in patients with CF in a fed state, the typical apparent volumes of distribution for the central and peripheral compartments [coefficient of variation as a percentage (CV)] were estimated to be 23.5 L (48.7%) and 33.3 L (30.5%), respectively. Ivacaftor is approximately 99% bound to plasma proteins, primarily to alpha 1-acid glycoprotein and albumin. After oral administration of ivacaftor 250 mg every 12 hours in combination with lumacaftor, the typical apparent volumes of distribution for the central and peripheral compartments (CV) were estimated to be 95.0 L (53.9%) and 201 L (26.6%), respectively.
In vitro studies indicate that lumacaftor is a substrate of Breast Cancer Resistance Protein (BCRP).
Lumacaftor is not extensively metabolised in humans, with the majority of lumacaftor excreted unchanged in the faeces. In vitro and in vivo data indicate that lumacaftor is mainly metabolised via oxidation and glucuronidation.
Ivacaftor is extensively metabolised in humans. In vitro and in vivo data indicate that ivacaftor is primarily metabolised by CYP3A. M1 and M6 are the two major metabolites of ivacaftor in humans. M1 has approximately one-sixth the potency of ivacaftor and is considered pharmacologically active. M6 has less than one-fiftieth the potency of ivacaftor and is not considered pharmacologically active.
Following oral administration of lumacaftor, the majority of lumacaftor (51%) is excreted unchanged in the faeces. There was negligible urinary excretion of lumacaftor as unchanged drug. The apparent terminal half-life is approximately 26 hours. The typical apparent clearance, CL/F (CV), of lumacaftor was estimated to be 2.38 L/h (29.4%) for patients with CF.
Following oral administration of ivacaftor alone, the majority of ivacaftor (87.8%) is eliminated in the faeces after metabolic conversion. There was negligible urinary excretion of ivacaftor as unchanged drug. In healthy subjects, the half-life of ivacaftor when given with lumacaftor is approximately 9 hours. The typical CL/F (CV) of ivacaftor when given in combination with lumacaftor was estimated to be 25.1 L/h (40.5%) for patients with CF.
Following multiple doses of lumacaftor/ivacaftor for 10 days, subjects with moderately impaired hepatic function (Child-Pugh Class B, score 7 to 9) had higher exposures (AUC0-12h by approximately 50% and Cmax by approximately 30%) compared with healthy subjects matched for demographics. The impact of mild hepatic impairment (Child-Pugh Class A, score 5 to 6) on pharmacokinetics of lumacaftor given in combination with ivacaftor has not been studied, but the increase in exposure is expected to be less than 50%.
Studies have not been conducted in patients with severe hepatic impairment (Child-Pugh Class C, score 10 to 15), but exposure is expected to be higher than in patients with moderate hepatic impairment (see sections 4.2, 4.4, and 4.8).
Pharmacokinetic studies have not been performed with lumacaftor/ivacaftor in patients with renal impairment. In a human pharmacokinetic study with lumacaftor alone, there was minimal elimination of lumacaftor and its metabolites in urine (only 8.6% of total radioactivity was recovered in the urine with 0.18% as unchanged parent). In a human pharmacokinetic study with ivacaftor alone, there was minimal elimination of ivacaftor and its metabolites in urine (only 6.6% of total radioactivity was recovered in the urine). A population pharmacokinetic analysis of clearance versus creatinine clearance shows no trend for subjects with mild and moderate renal impairment (see section 4.2).
The safety and efficacy of lumacaftor/ivacaftor in patients aged 65 years or older have not been evaluated.
The effect of gender on lumacaftor pharmacokinetics was evaluated using a population pharmacokinetics analysis of data from clinical studies of lumacaftor given in combination with ivacaftor. Results indicate no clinically relevant difference in pharmacokinetic parameters for lumacaftor or ivacaftor between males and females. No dose adjustments are necessary based on gender.
The exposures are similar between adults and the paediatric populations based on population PK analysis as presented in Table 11.
Table 11. Mean (SD) lumacaftor and ivacaftor exposure by age group:
| Age group | Weight | Dose | Mean lumacaftor (SD) AUCss (μgꞏh/mL) | Mean ivacaftor (SD) AUCss (μgꞏh/mL) |
|---|---|---|---|---|
| Patients aged 1 to <2 years | 7 kg to <9 kg N=1 | lumacaftor 75 mg/ivacaftor 94 mg sachet every 12 hours | 234 | 7.98 |
| 9 kg to <14 kg N=44 | lumacaftor 100 mg/ivacaftor 125 mg sachet every 12 hours | 191 (40.6) | 5.35 (1.61) | |
| ≥14 kg N=1 | lumacaftor 150 mg/ivacaftor 188 mg sachet every 12 hours | 116 | 5.82 | |
| Patients aged 2 to 5 years | <14 kg N=20 | lumacaftor 100 mg/ivacaftor 125 mg sachet every 12 hours | 180 (45.5) | 5.92 (4.61) |
| ≥14 kg N=42 | lumacaftor 150 mg/ivacaftor 188 mg sachet every 12 hours | 217 (48.6) | 5.90 (1.93) | |
| Patients aged 6 to <12 years | - N=62 | lumacaftor 200 mg/ivacaftor 250 mg every 12 hours | 203 (57.4) | 5.26 (3.08) |
| Patients aged 12 <18 years | - N=98 | lumacaftor 400 mg/ivacaftor 250 mg every 12 hours | 241 (61.4) | 3.90 (1.56) |
| Patients aged 18 years and older | - N=55 | Lumacaftor 400 mg/ivacaftor 250 mg every 12 hours | 198 (64.8) | 3.66 (2.25) |
Notes: Exposures for patients <18 years of age are from population PK analyses. Exposures for adult patients are from noncompartmental analyses.
Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, and toxicity to reproduction and development. Specific studies to evaluate the phototoxic potential of lumacaftor were not conducted; however, evaluation of the available non-clinical and clinical data suggests no phototoxic liability.
Effects in repeated dose studies were observed only at exposures considered sufficiently in excess (>25-, >45-, and >35-fold for mice, rats, and dogs, respectively) of the maximum human exposure of ivacaftor when administered as Orkambi, indicating little relevance to clinical use. Non-clinical data reveal no special hazard for humans based on conventional studies of genotoxicity and carcinogenic potential.
Ivacaftor produced concentration-dependent inhibitory effect on hERG (human ether-à-go-go related gene) tail currents, with an IC15 of 5.5 µM, compared to the Cmax (1.5 µM) for ivacaftor at the therapeutic dose for lumacaftor/ivacaftor. However, no ivacaftor-induced QT prolongation was observed in a dog telemetry study at single doses up to 60 mg/kg or in ECG measurements from repeat-dose studies of up to 1 year duration at the 60 mg/kg/day dose level in dogs (Cmax after 365 days = 36.2 to 47.6 μM). Ivacaftor produced a dose-related but transient increase in the blood pressure parameters in dogs at single oral doses up to 60 mg/kg (see section 5.1).
Ivacaftor was not teratogenic when dosed orally to pregnant rats and rabbits during the organogenesis stage of foetal development at doses approximately 7 times (ivacaftor and metabolite exposure) and 46 times the ivacaftor exposure in humans at the therapeutic lumacaftor/ivacaftor dose, respectively. At maternally toxic doses in rats, ivacaftor produced reductions in foetal body weight; an increase in the incidence of variations in cervical ribs, hypoplastic ribs, and wavy ribs; and sternal irregularities, including fusions. The significance of these findings for humans is unknown.
Ivacaftor impaired fertility and reproductive performance indices in male and female rats at 200 mg/kg/day (yielding exposures approximately 11 and 7 times, respectively, those obtained with the maximum recommended human dose of the ivacaftor component of Orkambi based on summed AUCs of ivacaftor and its metabolites extrapolated from day 90 exposures at 150 mg/kg/day in the 6-month repeat-dose toxicity study and gestation day 17 exposures in the pilot embryofoetal development study in this species) when dams were dosed prior to and during early pregnancy. No effects on male or female fertility and reproductive performance indices were observed at ≤100 mg/kg/day (yielding exposures approximately 8 and 5 times, respectively, those obtained with the maximum recommended human dose of the ivacaftor component of Orkambi based on summed AUCs of ivacaftor and its metabolites extrapolated from day 90 exposures at 100 mg/kg/day in the 6-month repeat-dose toxicity study and gestation day 17 exposures in the embryofoetal development study in this species). Placental transfer of ivacaftor was observed in pregnant rats and rabbits.
Ivacaftor did not cause developmental defects in the offspring of pregnant rats dosed orally from pregnancy through parturition and weaning at 100 mg/kg/day (yielding exposures that were approximately 4 times those obtained with the maximum recommended human dose of the ivacaftor component of Orkambi based on summed AUCs of ivacaftor and its metabolites). Doses above 100 mg/kg/day resulted in survival and lactation indices that were 92% and 98% of control values, respectively, as well as reductions in pup body weights.
Findings of cataracts were observed in juvenile rats dosed with ivacaftor at 0.32 times the maximum recommended human dose based on systemic exposure of ivacaftor and its metabolites when co-administered with lumacaftor as Orkambi. Cataracts were not observed in foetuses derived from rat dams treated during the organogenesis stage of foetal development, in rat pups exposed to a certain extent through milk ingestion prior to weaning, or in repeated dose toxicity studies with ivacaftor. The potential relevance of these findings in humans is unknown.
Repeat-dose toxicity studies involving the co-administration of lumacaftor and ivacaftor revealed no special hazard for humans in terms of potential for additive and/or synergistic toxicities.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.