PRESTALIA Tablet Ref.[50811] Active ingredients: Amlodipine Perindopril
Source: FDA, National Drug Code (US) Revision Year: 2019
1. Indications and Usage
PRESTALIA contains perindopril arginine, an angiotensin converting enzyme inhibitor, and amlodipine, a dihydropyridine calcium channel blocker, and is indicated for the treatment of hypertension, to lower blood pressure.
PRESTALIA may be used in patients whose blood pressure is not adequately controlled on monotherapy.
PRESTALIA may be used as initial therapy in patients likely to need multiple drugs to achieve blood pressure goals.
Lowering blood pressure reduces the risk of fatal and nonfatal cardiovascular events, primarily strokes and myocardial infarctions.
These benefits have been seen in controlled trials of antihypertensive drugs from a wide variety of pharmacologic classes, including amlodipine and the ACE inhibitor class to which perindopril principally belongs. There are no controlled trials demonstrating risk reduction with PRESTALIA.
Control of high blood pressure should be part of comprehensive cardiovascular risk management, including, as appropriate, lipid control, diabetes management, antithrombotic therapy, smoking cessation, exercise, and limited sodium intake. Many patients will require more than one drug to achieve blood pressure goals. For specific advice on goals and management, see published guidelines, such as those of the National High Blood Pressure Education Program's Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC).
Numerous antihypertensive drugs, from a variety of pharmacologic classes and with different mechanisms of action, have been shown in randomized controlled trials to reduce cardiovascular morbidity and mortality, and it can be concluded that it is blood pressure reduction, and not some other pharmacologic property of the drugs, that is largely responsible for those benefits. The largest and most consistent cardiovascular outcome benefit has been a reduction in the risk of stroke, but reductions in myocardial infarction and cardiovascular mortality also have been seen regularly.
Elevated systolic or diastolic pressure causes increased cardiovascular risk, and the absolute risk increase per mmHg is greater at higher blood pressures, so that even modest reductions of severe hypertension can provide substantial benefit. Relative risk reduction from blood pressure reduction is similar across populations with varying absolute risk, so the absolute benefit is greater in patients who are at higher risk independent of their hypertension (for example, patients with diabetes or hyperlipidemia), and such patients would be expected to benefit from more aggressive treatment to a lower blood pressure goal.
Some antihypertensive drugs have smaller blood pressure effects (as monotherapy) in black patients, and many antihypertensive drugs have additional approved indications and effects (e.g., on angina, heart failure, or diabetic kidney disease). These considerations may guide selection of therapy. In a clinical trial of PRESTALIA, treatment with PRESTALIA 14/10 mg did not provide additional antihypertensive effect beyond that achieved with use of amlodipine 10 mg in black and diabetic patients [see Clinical Studies (14)].
The choice of PRESTALIA as initial therapy for hypertension should be based on an assessment of potential benefits and risks including whether the patient is likely to tolerate the starting dose of PRESTALIA.
Patients with moderate-to-severe hypertension are at a relatively high risk of cardiovascular events (e.g., stroke, heart attack, and heart failure), kidney failure, and vision problems, so prompt treatment is clinically relevant. Consider the patient's baseline blood pressure, target goal and the incremental likelihood of achieving the goal with a combination product, such as PRESTALIA, versus a monotherapy product when deciding upon initial therapy. Individual blood pressure goals may vary based on the patient's risk.
Data from an 6-week, active-controlled trial provide estimates of the probability of reaching a target blood pressure with PRESTALIA compared with perindopril erbumine or amlodipine monotherapy [see Clinical Studies (14)].
Figures 1.a-1.d provide estimates of the likelihood of achieving target clinic systolic and diastolic blood pressure control with PRESTALIA 14/10 mg tablets after 6 weeks, based on baseline systolic and diastolic blood pressure. The curve for each treatment group was estimated by logistic regression modeling and is less well defined in the tails.
Figure 1.a Probability of Achieving Systolic Blood Pressure <140 mmHg at Week 6:
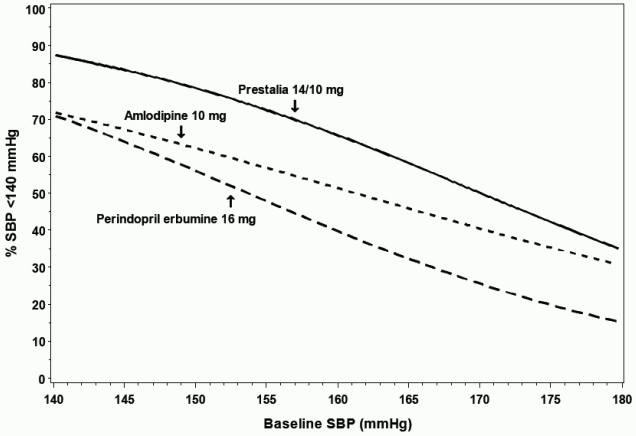
Figure 1.b Probability of Achieving Systolic Blood Pressure <130 mmHg at Week 6:

Figure 1.c Probability of Achieving Diastolic Blood Pressure <90 mmHg at Week 6:

Figure 1.d Probability of Achieving Diastolic Blood Pressure <80 mmHg at Week 6:
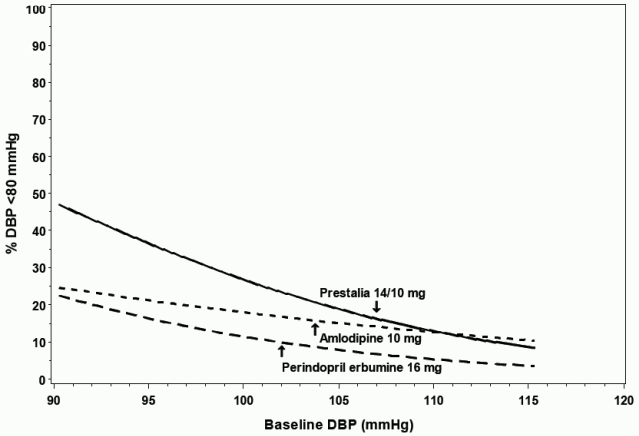
For example, a patient with a baseline blood pressure of 170/105 mmHg has approximately a 26% likelihood of achieving a goal of <140 mmHg (systolic) and 31% likelihood of achieving <90 mmHg (diastolic) on perindopril erbumine 16 mg. The likelihood of achieving these same goals on amlodipine 10 mg is approximately 40% (systolic) and 46% (diastolic). These likelihoods rise to 50% (systolic) and 65% (diastolic) with PRESTALIA 14/10 mg.
2. Dosage and Administration
2.1 General Considerations
The recommended starting dose of PRESTALIA is 3.5/2.5 mg once daily.
Adjust dosage according to blood pressure goals. In general, wait 7 to 14 days between titration steps. The maximum recommended dose is 14/10 mg once daily [see Clinical Pharmacology (12.3)].
PRESTALIA may be used as initial therapy if a patient is likely to need multiple drugs to achieve blood pressure goals. Consider use in patients unable to achieve adequate antihypertensive effect with amlodipine monotherapy because of dose-limiting peripheral edema caused by amlodipine [see Adverse Reactions (6)].
Administered as monotherapy, perindopril erbumine is an effective treatment for hypertension in once-daily doses ranging from 4 mg to 16 mg daily. Amlodipine is effective in once-daily doses of 5 mg and 10 mg. Adverse reactions related to perindopril are generally uncommon and independent of dose, while those related to amlodipine are a mixture of dose-dependent phenomena (primarily peripheral edema) and dose-independent phenomena, the former much more common than the latter [see Adverse Reactions (6)].
2.2 Dosage Adjustment in Renal Impairment
PRESTALIA is not recommended in patients with creatinine clearances <30 mL/min. For patients with creatinine clearance between 30 and 80 mL/min (mild or moderate renal impairment), do not exceed 7/5 mg [see Use in Specific Populations (8.6) and Warnings and Precautions (5.7)].
2.3 Monitoring in Elderly Patients (Over 65 Years of Age)
Monitor blood pressure for up to two weeks following titrations at dosages above 7/5 mg in patients over 65 years of age [see Use in Specific Populations (8.5) and Clinical Pharmacology (12.3)].
10. Overdosage
Perindopril
In animals, doses of perindopril up to 2,500 mg/kg in mice, 3,000 mg/kg in rats and 1,600 mg/kg in dogs were non-lethal. Past experiences were scant but suggested that overdosage with other ACE inhibitors was also fairly well tolerated by humans. The most likely manifestation is hypotension, and treatment should be symptomatic and supportive. Therapy with the ACE inhibitor should be discontinued, and the patient should be observed. Dehydration, electrolyte imbalance and hypotension should be treated by established procedures.
Among the reported cases of perindopril overdosage, patients who were known to have ingested a dose of 80 mg to 120 mg required assisted ventilation and circulatory support. One additional patient developed hypothermia, circulatory arrest and died following ingestion of up to 180 mg of perindopril. The intervention for perindopril overdose may require vigorous support.
Laboratory determinations of serum levels of perindopril and its metabolites are not widely available, and such determinations have, in any event, no established role in the management of perindopril overdose. No data are available to suggest physiological maneuvers (e.g., maneuvers to change the pH of the urine) that might accelerate elimination of perindopril and its metabolites.
Angiotensin II could presumably serve as a specific antagonist-antidote in the settling of perindopril overdose, but angiotensin II is essentially unavailable outside of scattered research facilities. Because the hypotensive effect of perindopril is achieved through vasodilation and effective hypovolemia, it is reasonable to treat perindopril overdose by infusion of normal saline solution.
Amlodipine
Overdosage might be expected to cause excessive peripheral vasodilation with marked hypotension and possibly a reflex tachycardia. In humans, experience with intentional overdosage of amlodipine is limited.
Single oral doses of amlodipine maleate equivalent to 40 mg amlodipine/kg and 100 mg amlodipine/kg in mice and rats, respectively, caused deaths. Single oral amlodipine maleate doses equivalent to 4 or more mg amlodipine/kg or higher in dogs (11 or more times the maximum recommended human dose on a mg/m 2 basis) caused a marked peripheral vasodilation and hypotension.
If massive overdose should occur, initiate active cardiac and respiratory monitoring. Frequent blood pressure measurements are essential. Should hypotension occur, provide cardiovascular support including elevation of the extremities and the judicious administration of fluids. If hypotension remains unresponsive to these conservative measures, consider administration of vasopressors (such as phenylephrine) with attention to circulating volume and urine output. As amlodipine is highly protein bound, hemodialysis is not likely to be of benefit.
16.2. Storage and Handling
Store at 25°C (77°F); excursions permitted to 15-30°C (59-86°F). [See USP controlled room temperature.] Protect from moisture. Dispense in tight container (USP).
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.