SAPHRIS Tablet Ref.[27430] Active ingredients: Asenapine
Source: FDA, National Drug Code (US) Revision Year: 2017
12.1. Mechanism of Action
The mechanism of action of asenapine, in schizophrenia and bipolar I disorder, is unknown. It has been suggested that the efficacy of asenapine in schizophrenia could be mediated through a combination of antagonist activity at D2 and 5-HT2A receptors.
12.2. Pharmacodynamics
Asenapine exhibits high affinity for serotonin 5-HT1A, 5-HT1B, 5-HT2A, 5-HT2B, 5-HT2C, 5-HT5A, 5-HT6 and 5-HT7 receptors (Ki values of 2.5, 2.7, 0.07, 0.18, 0.03, 1.6, 0.25, and 0.11 nM, respectively), dopamine D2A, D2B, D3, D4, and D1 receptors (Ki values of 1.3, 1.4, 0.42, 1.1, and 1.4 nM, respectively), α1A, α2A, α2B, and α2C-adrenergic receptors (Ki values of 1.2, 1.2, 0.33 and 1.2 nM, respectively), and histamine H1 receptors (Ki value 1.0 nM), and moderate affinity for H2 receptors (Ki value of 6.2 nM). In in vitro assays asenapine acts as an antagonist at these receptors. Asenapine has no appreciable affinity for muscarinic cholinergic receptors (e.g., Ki value of 8128 nM for M1).
12.3. Pharmacokinetics
Following a single 5 mg dose of SAPHRIS, the mean Cmax was approximately 4 ng/mL and was observed at a mean tmax of 1 hour. Elimination of asenapine is primarily through direct glucuronidation by UGT1A4 and oxidative metabolism by cytochrome P450 isoenzymes (predominantly CYP1A2). Following an initial more rapid distribution phase, the mean terminal half-life is approximately 24 hrs. With multiple-dose twice-daily dosing, steady-state is attained within 3 days. Overall, steady-state asenapine pharmacokinetics are similar to single-dose pharmacokinetics.
Absorption
Following sublingual administration, asenapine is rapidly absorbed with peak plasma concentrations occurring within 0.5 to 1.5 hours. The absolute bioavailability of sublingual asenapine at 5 mg is 35%. Increasing the dose from 5 mg to 10 mg twice daily (a two-fold increase) results in less than linear (1.7 times) increases in both the extent of exposure and maximum concentration. The absolute bioavailability of asenapine when swallowed is low (<2% with an oral tablet formulation).
The intake of water several (2 or 5) minutes after asenapine administration resulted in decreased asenapine exposure. Therefore, eating and drinking should be avoided for 10 minutes after administration [see Dosage and Administration (2.1)].
Distribution
Asenapine is rapidly distributed and has a large volume of distribution (approximately 20-25 L/kg), indicating extensive extravascular distribution. Asenapine is highly bound (95%) to plasma proteins, including albumin and α1-acid glycoprotein.
Metabolism and Elimination
Direct glucuronidation by UGT1A4 and oxidative metabolism by cytochrome P450 isoenzymes (predominantly CYP1A2) are the primary metabolic pathways for asenapine.
Asenapine is a high clearance drug with a clearance after intravenous administration of 52 L/h. In this circumstance, hepatic clearance is influenced primarily by changes in liver blood flow rather than by changes in the intrinsic clearance, i.e., the metabolizing enzymatic activity. Following an initial more rapid distribution phase, the terminal half-life of asenapine is approximately 24 hours. Steady-state concentrations of asenapine are reached within 3 days of twice daily dosing.
After administration of a single dose of [14C]-labeled asenapine, about 90% of the dose was recovered; approximately 50% was recovered in urine, and 40% recovered in feces. About 50% of the circulating species in plasma have been identified. The predominant species was asenapine N +-glucuronide; others included N-desmethylasenapine, N-desmethylasenapine N-carbamoyl glucuronide, and unchanged asenapine in smaller amounts. SAPHRIS activity is primarily due to the parent drug.
In vitro studies indicate that asenapine is a substrate for UGT1A4, CYP1A2 and to a lesser extent CYP3A4 and CYP2D6. Asenapine is a weak inhibitor of CYP2D6. Asenapine does not cause induction of CYP1A2 or CYP3A4 activities in cultured human hepatocytes. Coadministration of asenapine with known inhibitors, inducers or substrates of these metabolic pathways has been studied in a number of drug-drug interaction studies [see Drug Interactions (7.1)].
Food
A crossover study in 26 healthy adult male subjects was performed to evaluate the effect of food on the pharmacokinetics of a single 5 mg dose of asenapine. Consumption of food immediately prior to sublingual administration decreased asenapine exposure by 20%; consumption of food 4 hours after sublingual administration decreased asenapine exposure by about 10%. These effects are probably due to increased hepatic blood flow.
In clinical trials establishing the efficacy and safety of SAPHRIS, patients were instructed to avoid eating for 10 minutes following sublingual dosing. There were no other restrictions with regard to the timing of meals in these trials [see Dosage and Administration (2.1)].
Water
In clinical trials establishing the efficacy and safety of SAPHRIS, patients were instructed to avoid drinking for 10 minutes following sublingual dosing. The effect of water administration following 10 mg sublingual SAPHRIS dosing was studied at different time points of 2, 5, 10, and 30 minutes in 15 healthy adult male subjects. The exposure of asenapine following administration of water 10 minutes after sublingual dosing was equivalent to that when water was administered 30 minutes after dosing. Reduced exposure to asenapine was observed following water administration at 2 minutes (19% decrease) and 5 minutes (10% decrease) [see Dosage and Administration (2.1)].
Drug Interaction Studies
Effects of other drugs on the exposure of asenapine are summarized in Figure 1. In addition, a population pharmacokinetic analysis indicated that the concomitant administration of lithium had no effect on the pharmacokinetics of asenapine.
Figure 1. Effect of Other Drugs on Asenapine Pharmacokinetics:

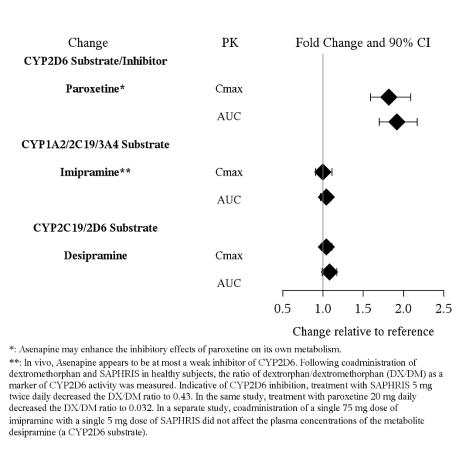
The effects of asenapine on the pharmacokinetics of other co-administered drugs are summarized in Figure 2.
Coadministration of paroxetine with SAPHRIS caused a two-fold increase in the maximum plasma concentrations and systemic exposure of paroxetine. Asenapine enhances the inhibitory effects of paroxetine on its own metabolism by CYP2D6.
Figure 2. Effect of Asenapine on Other Drug Pharmacokinetics:
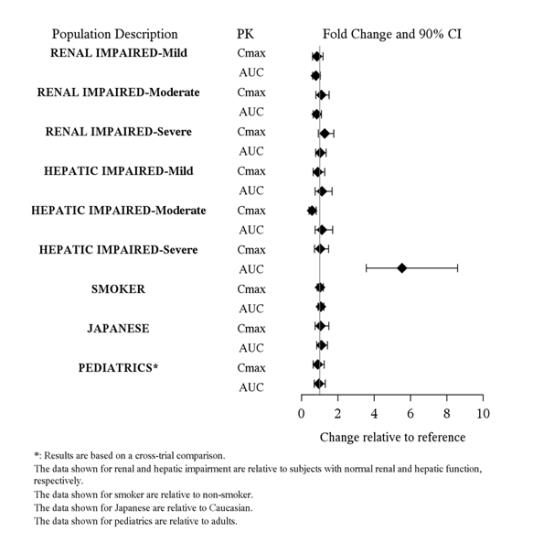
Studies in Special Populations
Exposures of asenapine in special populations are summarized in Figure 3. Additionally, based on population pharmacokinetic analysis, no effects of sex, race, BMI, and smoking status on asenapine exposure were observed. Exposure in elderly patients is 30-40% higher as compared to adults.
Figure 3. Effect of Intrinsic Factors on Asenapine Pharmacokinetics:
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
In a lifetime carcinogenicity study in CD-1 mice asenapine was administered subcutaneously at doses up to those resulting in plasma levels (AUC) estimated to be 5 times those in humans receiving the MRHD of 10 mg twice daily. The incidence of malignant lymphomas was increased in female mice, with a no-effect dose resulting in plasma levels estimated to be 1.5 times those in humans receiving the MRHD. The mouse strain used has a high and variable incidence of malignant lymphomas, and the significance of these results to humans is unknown. There were no increases in other tumor types in female mice. In male mice, there were no increases in any tumor type.
In a lifetime carcinogenicity study in Sprague-Dawley rats, asenapine did not cause any increases in tumors when administered subcutaneously at doses up to those resulting in plasma levels (AUC) estimated to be 5 times those in humans receiving the MRHD.
Mutagenesis
No evidence for genotoxic potential of asenapine was found in the in vitro bacterial reverse mutation assay, the in vitro forward gene mutation assay in mouse lymphoma cells, the in vitro chromosomal aberration assays in human lymphocytes, the in vitro sister chromatid exchange assay in rabbit lymphocytes, or the in vivo micronucleus assay in rats.
Impairment of Fertility
Asenapine did not impair fertility in rats when tested at doses up to 11 mg/kg twice daily given orally. This dose is 10 times the maximum recommended human dose of 10 mg twice daily given sublingually on a mg/m² basis.
14. Clinical Studies
Efficacy of SAPHRIS was established in the following trials:
- Two fixed-dose, short-term trials and one flexible-dose, maintenance trial in adult patients with schizophrenia as monotherapy [see Clinical Studies (14.1)]
- One fixed-dose and two flexible-dose, short-term trials of monotherapy in adults with manic or mixed episodes associated with bipolar I disorder [see Clinical Studies (14.2)]
- One flexible-dose, maintenance trial of monotherapy in adults with bipolar I disorder [see Clinical Studies (14.2)]
- One fixed-dose, short term trial of monotherapy in children (10 to 17 years) with manic or mixed episodes associated with bipolar I disorder [see Clinical Studies (14.2)]
- One flexible-dose, short-term trial in adult patients with manic or mixed episode associated with bipolar I disorder as adjunctive treatment to lithium or valproate [see Clinical Studies (14.2)]
14.1 Schizophrenia
The efficacy of SAPHRIS in the treatment of schizophrenia in adults was evaluated in three fixed-dose, short-term (6 week), randomized, double-blind, placebo-controlled, and active-controlled (haloperidol, risperidone, and olanzapine) trials of adult patients who met DSM-IV criteria for schizophrenia and were having an acute exacerbation of their schizophrenic illness. In two of the three trials SAPHRIS demonstrated superior efficacy to placebo. In a third trial, SAPHRIS could not be distinguished from placebo; however, an active control in that trial was superior to placebo.
In the two positive trials for SAPHRIS, the primary efficacy rating scale was the Positive and Negative Syndrome Scale (PANSS). The PANSS is a 30 item scale that measures positive symptoms of schizophrenia (7 items), negative symptoms of schizophrenia (7 items), and general psychopathology (16 items), each rated on a scale of 1 (absent) to 7 (extreme); total PANSS scores range from 30 to 210. The primary endpoint was change from baseline to endpoint on the PANSS total score. The results of the SAPHRIS trials in schizophrenia follow:
In trial 1, a 6-week trial (n=174), comparing SAPHRIS (5 mg twice daily) to placebo, SAPHRIS 5 mg twice daily was statistically superior to placebo on the PANSS total score (Trial 1 in Table 13).
In trial 2, a 6-week trial (n=448), comparing two fixed doses of SAPHRIS (5 mg and 10 mg twice daily) to placebo, SAPHRIS 5 mg twice daily was statistically superior to placebo on the PANSS total score. SAPHRIS 10 mg twice daily showed no added benefit compared to 5 mg twice daily and was not significantly different from placebo (Trial 2 in Table 13).
An examination of population subgroups did not reveal any clear evidence of differential responsiveness on the basis of age, sex or race.
Table 13. Short-Term Schizophrenia Trials Establishing Efficacy in Adults:
| Trial Number | Treatment Group | Primary Efficacy Measure: PANSS Total Score | ||
|---|---|---|---|---|
| Mean Baseline Score (SD) | LS Mean Change from Baseline (SE) | Placebo-subtracted Difference a (95% CI) | ||
| Trial 1 | SAPHRIS 5 mg* twice daily | 96.5 (16.4) | -14.4 (2.6) | -9.7 (-17.6, -1.8) |
| Placebo | 92.4 (14.9) | -4.6 (2.5) | -- | |
| Trial 2 | SAPHRIS 5 mg* twice daily | 89.2 (12.0) | -16.2 (1.7) | -5.5 (-10.7, -0.2) |
| SAPHRIS 10 mg twice daily | 89.1 (12.9) | -14.9 (1.7) | -4.1 (-9.4, 1.2) | |
| Placebo | 88.9 (11.7) | -10.7 (1.6) | -- | |
SD: standard deviation; SE: standard error; LS Mean: least-squares mean; CI: confidence interval, not adjusted for multiple comparisons.
a Difference (drug minus placebo) in least-squares mean change from baseline.
* Doses that are demonstrated to be effective.
Maintenance of efficacy has been demonstrated in a placebo-controlled, double-blind, multicenter, flexible dose (5 mg or 10 mg twice daily based on tolerability) clinical trial with a randomized withdrawal design. All patients were initially administered 5 mg twice daily for 1 week and then titrated up to 10 mg twice daily. A total of 700 patients entered open-label treatment with SAPHRIS for a period of 26 weeks. Of these, a total of 386 patients who met pre-specified criteria for continued stability (mean length of stabilization was 22 weeks) were randomized to a double-blind, placebo-controlled, randomized withdrawal phase. SAPHRIS was statistically superior to placebo in time to relapse or impending relapse defined as increase in PANSS ≥20% from baseline and a Clinical Global Impression–Severity of Illness (CGI-S) score ≥4 (at least 2 days within 1 week) or PANSS score ≥5 on "hostility" or "uncooperativeness" items and CGI-S score ≥4 (≥2 days within a week), or PANSS score ≥5 on any two of the following items: "unusual thought content", "conceptual disorganization", or "hallucinatory behavior" items, and CGI-S score ≥4 (≥2 days within 1 week) or investigator judgment of worsening symptoms or increased risk of violence to self (including suicide) or other persons. The Kaplan-Meier curves of the time to relapse or impending relapse during the double-blind, placebo-controlled, randomized withdrawal phase of this trial for SAPHRIS and placebo are shown in Figure 4.
Figure 4. Kaplan-Meier Estimation of Percent Relapse/Impending Relapse for SAPHRIS and placebo:

14.2 Bipolar I Disorder
Monotherapy
Adults
The efficacy of SAPHRIS in the treatment of acute mania was established in two similarly designed 3-week, randomized, double-blind, placebo-controlled, and active-controlled (olanzapine) trials of adult patients who met DSM-IV criteria for Bipolar I Disorder with an acute manic or mixed episode with or without psychotic features.
The primary rating instrument used for assessing manic symptoms in these trials was the Young Mania Rating Scale (YMRS), an 11-item clinician-rated scale traditionally used to assess the degree of manic symptomatology in a range from 0 (no manic features) to 60 (maximum score). Patients were also assessed on the Clinical Global Impression – Bipolar (CGI-BP) scale. In both trials, all patients randomized to SAPHRIS were initially administered 10 mg twice daily, and the dose could be adjusted within the dose range of 5 to 10 mg twice daily from Day 2 onward based on efficacy and tolerability. Ninety percent of patients remained on the 10 mg twice daily dose. SAPHRIS was statistically superior to placebo on the YMRS total score and the CGI-BP Severity of Illness score (mania) in both studies (Trials 1 and 2 in Table 14).
In another 3-week, randomized, double-blind, placebo-controlled trial (n=359), comparing two fixed doses of SAPHRIS (5 mg and 10 mg twice daily) to placebo, both doses were statistically superior to placebo on the YMRS total score and CGI-BP Severity of Illness overall score. (Trial 3 in Table 14).
An examination of subgroups did not reveal any clear evidence of differential responsiveness on the basis of age, sex, or race.
Maintenance of efficacy has been demonstrated in a placebo-controlled, double-blind, multicenter, flexible dose (5 mg or 10 mg twice daily based on tolerability) clinical trial with a randomized withdrawal design. All patients were initially administered 5 or 10 mg twice daily, and the option to titrate down to 5 mg twice daily was provided based on tolerability. A total of 549 patients entered open-label treatment with SAPHRIS for a period of 12 to16 weeks. Of these, a total of 252 patients who met pre-specified criteria for continued stability were randomized to and treated in a double-blind, placebo-controlled, randomized withdrawal phase. SAPHRIS was statistically superior to placebo in time to relapse defined as 1) YMRS or MADRS score ≥16; 2) requirement or initiation of any non-study medication to treat mixed, manic, or depressive symptoms, including an antipsychotic, antidepressant, or mood-stabilizing agent; 3) requirement or initiation of psychiatric hospitalization; 4) investigator judgment to discontinue the study due to a mood event. The Kaplan-Meier curves of the time to relapse during the double-blind, placebo-controlled, randomized withdrawal phase of this trial for SAPHRIS and placebo are shown in Figure 5.
Figure 5. Kaplan-Meier Estimation of Percent Relapse for SAPHRIS and Placebo:

Time (days) represents the number of days from randomization in the double-blind period to the first date of achieving relapse status.
The product limit estimators are based on the Kaplan-Meier distribution with censoring at last contact date.
Pediatric patients
The efficacy of SAPHRIS in the treatment of acute mania was established in a single, 3-week, placebo-controlled, double-blind trial of 403 pediatric patients 10 to 17 years of age, of whom 302 patients received SAPHRIS at fixed doses of 2.5 mg, 5 mg and 10 mg twice daily. All patients were started on 2.5 mg twice daily. For those assigned to 5 mg twice daily, the dose was increased to 5 mg twice daily after 3 days. For those assigned to 10 mg twice daily, the dose was increased from 2.5 to 5 mg twice daily after 3 days, and then to 10 mg twice daily after 3 additional days.
SAPHRIS was statistically superior to placebo in improving YMRS total score and the CGI-BP Severity of Illness overall score as measured by the change from baseline to week 3 (Trial 3 Pediatric in Table 14). An examination of subgroups did not reveal any clear evidence of differential responsiveness on the basis of age, sex, and race.
Adjunctive Therapy: The efficacy of SAPHRIS as an adjunctive therapy in acute mania was established in a 12-week, placebo-controlled trial with a 3-week primary efficacy endpoint involving 326 adult patients with a manic or mixed episode of Bipolar I Disorder, with or without psychotic features, who were partially responsive to lithium or valproate monotherapy after at least 2 weeks of treatment. All patients randomized to SAPHRIS were initially administered 5 mg twice daily, and the dose could be adjusted within the dose range of 5 to 10 mg twice daily from Day 2 onward based on efficacy and tolerability. SAPHRIS was statistically superior to placebo in the reduction of manic symptoms (measured by the YMRS total score) as an adjunctive therapy to lithium or valproate monotherapy at Week 3 (Trial 5 Adjunctive in Table 14).
Table 14. Acute Bipolar I Trials Establishing Efficacy in Adults and Pediatric Patients 10 to 17 Years:
| Study Number | Treatment Group | Primary Efficacy Measure: YMRS Total Score | ||
|---|---|---|---|---|
| Mean Baseline Score (SD) | LS Mean Change from Baseline (SE) | Placebo-subtracted Differencea (95% CI) | ||
| Trial 1 | SAPHRIS 5-10 mg* twice daily | 29.4 (6.7) | -11.5 (0.8) | -3.7 (-6.6, -0.7) |
| Placebo | 28.3 (6.3) | -7.8 (1.1) | -- | |
| Trial 2 | SAPHRIS 5-10 mg* twice daily | 28.3 (5.5) | -10.8 (0.8) | -5.3 (-8.0, -2.5) |
| Placebo | 29.0 (6.1) | -5.5 (1.0) | -- | |
| Trial 3 | SAPHRIS 5 mg* twice daily SAPHRIS 10 mg* twice daily Placebo | 29.7 (5.9) 30.2 (5.4) 30.0 (5.6) | -14.4 (1.0) -14.9 (1.0) -10.9 (1.0) | -4.0 (-6.9, -1.2) |
| Trial 4 (Pediatric 10 to 17 years) | SAPHRIS 2.5 mg* twice daily | 29.5 (5.7) | -12.8 (0.8) | -3.2 (-5.6, -0.8) |
| SAPHRIS 5 mg* twice daily | 30.4 (5.9) | -14.9 (0.8) | -5.3 (-7.7, -2.9) | |
| SAPHRIS 10 mg* twice daily | 30.1 (5.7) | -15.8 (0.9) | -6.2 (-8.6, -3.8) | |
| Placebo | 30.1 (5.7) | - 9.6 (0.9) | -- | |
| Trial 5 (Adjunctive) | SAPHRIS 5-10 mg* twice daily + lithium/ Valproate | 28.0 (5.6) | -10.3 (0.8) | -2.4 (-4.4, -0.3) |
| Lithium/Valproate | 28.2 (5.8) | -7.9 (0.8) | -- | |
SD: standard deviation; SE: standard error; LS Mean: least-squares mean; CI: confidence interval, not adjusted for multiple comparisons.
a Difference (drug minus placebo) in least-squares mean change from baseline.
* Doses that are demonstrated to be effective.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.