TYLENOL Tablets, Capsule, Suspension, Powder Ref.[50413] Active ingredients: Paracetamol
Source: Health Products and Food Branch (CA) Revision Year: 2021
Contraindications
Hypersensitivity to acetaminophen or to the ingredients of this formulation (see Dosage Forms, Composition and Packaging). Allergic reactions (primarily skin rash) or reports of hypersensitivity secondary to acetaminophen are rare and generally are controlled by discontinuation of the drug and, when necessary, symptomatic treatment. Do not use with any other product containing acetaminophen.
Warnings and precautions
General
Adults and children 12 years and older should not exceed 4 g/day of acetaminophen or use more than one product containing acetaminophen at a time. Children under 12 years should not be given more than the maximum daily dosage stated on the product label. These limits include combination products that contain acetaminophen.
Overdose warning
Taking more than the recommended dose (overdose) may result in liver damage. In case of overdose, get medical help right away. Quick medical attention is critical for adults as well as for children even if you do not notice any signs or symptoms.
Acetaminophen-containing products should be kept out of the reach of children.
Consumers who are chronic alcohol abusers or have hepatic disease should ask their doctor whether they should take acetaminophen or other pain relievers or fever reducers. Physicians should be cognizant of and supervise the use of acetaminophen in patients with chronic alcoholism, serious kidney or serious liver disease. Physicians should alert their patients who regularly consume large amounts of alcohol not to exceed the recommended doses of acetaminophen. Chronic heavy alcohol abusers may be at increased risk of liver toxicity from excessive doses of acetaminophen.
Patients should be counseled to stop use and consult a physician if redness or swelling is present in an area of pain, if symptoms do not improve or if they worsen; if pain or fever persists or gets worse; or if new symptoms such as high fever, rash, itching or persistent headache occur, as these may be signs of a condition which requires medical attention.
Acetaminophen should not be taken for pain for more than 5 days, for fever for more than 3 days or if new symptoms appear, without consulting a physician.
Hepatic
Slower metabolism of acetaminophen, increased activity of the cytochrome P450 enzyme system, or depleted glutathione stores are cited as theoretical risk factors for acetaminophen hepatotoxicity in patients with chronic liver disease. However, acetaminophen has been studied in both adults and children with a wide variety of liver diseases including various types of cirrhosis, hepatitis (including hepatitis C), nodular transformation, congenital hepatic fibrosis, and α1-antitrypsin deficiency. In none of these conditions is there evidence of an increased risk for hepatotoxicity at currently recommended acetaminophen doses but the studies were insufficiently powered to definitely establish the extent of risk. Patients with hepatic disease should consult a physician before use.
Forrest1 compared acetaminophen metabolism following a single 1500 mg dose in normal subjects, patients with mild liver disease, and patients with severe liver disease. There were no significant differences in overall 24-hour urinary excretion of acetaminophen and glucuronide, sulfate, cysteine, and mercapturic acid conjugates, evidence that acetaminophen metabolism was similar to that in normal subjects. However, the elimination half-life was significantly prolonged in patients with severe liver disease.
Acetaminophen has also been studied in pediatric patients with liver disease. Following a single (10 mg/kg) dose of acetaminophen, the pharmacokinetic profiles in pediatric patients with mild, moderate, or severe liver disease were not significantly different2. Although the plasma half-life of acetaminophen was prolonged in patients with severe liver disease, there were no significant differences in the 36-hour (children) urinary excretion of acetaminophen or its conjugates.
At the currently recommended doses acetaminophen is a suitable analgesic choice for use in patients with chronic stable liver disease when used under physician supervision.
Acetaminophen may cause hepatotoxicity in situations of intentional overdose (e.g. attempted suicide), unintentional overdose (e.g. overdosing when pain relief is not satisfactory), simultaneous use of multiple acetaminophen-containing preparations, accidental overdose or in very rare cases, after recommended doses, although causality has not been determined. The hepatotoxic reaction can be severe and life-threatening. Early symptoms following a hepatotoxic overdose may include nausea, vomiting, diaphoresis, lethargy, and general malaise. If appropriate treatment is not instituted, these may progress to upper quadrant pain, confusion, stupor, and sequelae of hepatic necrosis, such as jaundice, coagulation defects, hypoglycemia, and encephalopathy. Renal failure and cardiomyopathy may also occur. In the event of known or suspected overdosage, treatment with N-acetyl cysteine should be instituted immediately (see OVERDOSAGE section below), even when there are no obvious symptoms. Failure to promptly treat acetaminophen hepatotoxicity with N-acetyl cysteine can result in liver failure, leading to liver transplantation and/or death.
Chronic Alcohol Use
Excessive alcohol use may increase risk of liver toxicity from acetaminophen overdose (acute or chronic)3-5.
Prospective data from Kuffner5,6 demonstrate that chronic alcoholics can take recommended doses of acetaminophen without the added risk of liver injury. In these prospective, placebo-controlled studies, the researchers evaluated an actively drinking group of alcoholics with a high prevalence of malnourishment. The study participants abruptly stopped their daily alcohol intake and took acetaminophen the next day. This should theoretically make them vulnerable to acetaminophen injury because their CYP2E1 would be maximally induced from the alcohol and there would be no alcohol present to compete with acetaminophen for metabolism by CYP2E1. There was no statistically significant difference in mean values for AST, ALT, or INR for alcoholics given four grams per day of acetaminophen compared to placebo. Additionally, the researchers performed an analysis of the malnourished patients that showed there was no increase in AST or ALT levels in these patients. Study limitations include a limited duration of 2 days and exclusion of patients with preexisting AST or ALT elevations greater than 120 U/L. Study results do not preclude the possibility of an idiosyncratic hepatic reaction.
Renal
Based on available clinical data, acetaminophen can be used in patients with chronic renal disease without dosage adjustment. Martin7 found that patients with chronic renal failure had higher plasma concentrations of acetaminophen and the inactive glucuronide and sulfate metabolites than healthy subjects during repeated dosing up to ten days.
Several single-dose studies demonstrate accumulation of acetaminophen metabolites in patients with moderate chronic renal failure and in anephric patients8-10 for whom hemodialysis appeared to be the major route of elimination11.
The habitual consumption of acetaminophen should be discouraged. If indicated medically, the long-term use of acetaminophen should be supervised by a physician.
A National Kidney Foundation position paper notes that physicians preferentially recommend acetaminophen to patients with renal failure because of the bleeding complications associated with ASA in these individuals12. Acetaminophen was recommended as the non-narcotic analgesic of choice for episodic use in patients with underlying renal disease.
Skin
Serious skin reactions such as acute generalized exanthematous pustulosis (AGEP), Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN), have been reported very rarely in patients receiving acetaminophen. Patients should be informed about the signs of serious skin reactions, and use of the drug should be discontinued at the first appearance of skin rash or any other sign of hypersensitivity.
Special Populations
Notwithstanding appropriate precautions, acetaminophen is a suitable analgesic choice for the majority of sub-populations at increased risk of adverse events from analgesic use. This includes asthmatics, elderly, patients taking multiple prescription drugs, patients taking anti-coagulants, patients who are breast-feeding, as well as patients who may suffer from chronic alcoholism, serious kidney or liver disease.
Results of well-designed clinical studies indicate that a dose reduction of acetaminophen, to avoid potential increased risk for toxicity, is not necessary for elderly adults, and obese adults. Additionally, the weight of existing evidence does not indicate the need to adjust dosage in chronic renal disease or chronic stable liver disease.
Elderly Patients
Acetaminophen at currently recommended doses can be used safely by elderly patients. Results of well-designed clinical studies indicate that a dose reduction of acetaminophen, to avoid potential increased risk for toxicity, is not necessary. In a comprehensive metabolic study by Miners13, the formation and clearance of glucuronide and glutathione conjugates were the same in young and elderly adults, although clearance of the sulphate conjugate and unchanged acetaminophen were reduced. This finding provides prospective scientific data that the amount of acetaminophen metabolized via the oxidative pathway, from which the highly reactive intermediate, NAPQI, is generated, does not increase with age. Recently, Bannwarth14 evaluated the multipledose pharmacokinetics of acetaminophen in elderly patients. After seven days of repeat dosing, acetaminophen did not accumulate in the plasma, and the elimination half-life was the same as that reported for young adults.
Elderly patients who require therapy for longer than 5 days should consult their physician for condition monitoring; however, no reduction in recommended dosage is necessary. The American Geriatrics Society Clinical Practice Guidelines for the Management of Chronic Pain in Older Persons15 recommend acetaminophen as the drug of choice for relieving mild to moderate musculoskeletal pain, with the maximum dosage not to exceed 4000 mg daily. Acetaminophen is safe for use in the elderly population as currently labeled.
Glucose-6-Phosphate Dehydrogenase (G6PD) Deficiency
In therapeutic doses, acetaminophen does not shorten the lifespan of red blood cells16,17 and does not produce any clinically perceptible destruction of circulating red blood cells18.
Obese Adults
Results of well-designed clinical studies indicate that a dose reduction of acetaminophen, to avoid potential increased risk for toxicity, is not necessary. O'Shea19 studied the pharmacokinetics of chlorzoxazone (a putative probe for CYP2E1 activity) to evaluate the effect of obesity on CYP2E1 activity. The authors concluded that CYP2E1 is induced in obese adults and that this could impact the metabolic pathway of a number of drugs metabolized by CYP2E1, including acetaminophen. However, acetaminophen pharmacokinetic data have been investigated in obese adults20. In this prospective study, 650 mg acetaminophen was administered intravenously to obese men (297 lb), obese women (193 lb), control men (155 lb) and control women (121 lb). Acetaminophen distribution volume per total body weight was slightly lower in the obese adults but, more importantly, the half-life and metabolic clearance per total body weight did not differ among groups.
Pregnancy and Lactation
There are no adequate and well controlled clinical studies in pregnant or breast-feeding women.
Adverse reactions
Central Nervous System Effects
Acetaminophen at recommended doses has no obvious effects on central nervous system function21. In an overdose situation, central nervous system effects are uncommon.
Gastrointestinal Effects
Acetaminophen at recommended doses does not cause gastric irritation, gastric erosions, occult or overt gastrointestinal blood loss or ulcers22,23.
Blot and McLaughlin24 conducted an independent analysis of case-control data from a study conducted by the American College of Gastroenterology. The risk of gastrointestinal bleeding increased two to three-fold among recent users of ASA, ibuprofen and other NSAIDs at OTC doses, and the risk was also dose-related. In contrast, the use of acetaminophen was not associated with an increased risk of gastrointestinal bleeding.
Hematologic Effects
Acetaminophen does not have any immediate or delayed effects on small vessel hemostasis, as measured by bleeding time. In normal volunteers receiving a single dose of acetaminophen (975 or 1950 mg) or multiple doses of acetaminophen (1950 mg daily for 6 weeks), no change in bleeding time or platelet aggregation was observed25. In another study, a single 1000 mg dose of acetaminophen was given to normal volunteers and did not affect bleeding time or platelet aggregation26. Patients with hemophilia receiving multiple doses of acetaminophen showed no significant changes in bleeding time27,28.
Haematological reactions including thrombocytopenia, leucopenia, pancytopenia, neutropenia, and agranulocytosis have been reported, although these are rare and causality has not been established.
Hepatic Effects
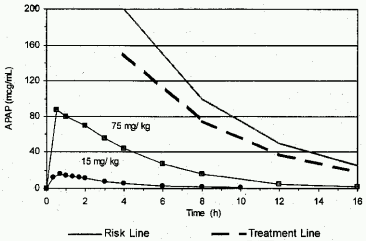
As an illustration of the margin of safety of acetaminophen at supratherapeutic doses, a comparison of serum concentrations of acetaminophen over time for a standard 15 mg/kg dose and for a dose exceeding the standard by a multiple of 5 (75 mg/kg) are shown in Figure 1. The serum concentrations are drawn relative to the risk line for hepatotoxicity and treatment line of the Rumack-Matthew nomogram used to manage acute overdoses. The mean plasma concentrations for this supratherapeutic dose are well below the risk and treatment lines of the nomogram at all times. However, to minimize the risk for adverse effects, the maximum recommended dose should not be exceeded.
Figure 1. Mean Data for a Standard (1 g, 15 mg/kg) and Higher (5.6 g, 75 mg/kg) Dose Relative to Risk and Treatment Lines of the Acetaminophen Nomogram:
Acetaminophen in overdosage may cause hepatotoxicity. In adults and adolescents, hepatotoxicity may occur following ingestion of greater than 150 mg/kg over a period of 8 hours or less. Fatalities are infrequent (less than 3% to 4% of untreated cases in which blood levels exceed the treatment line) and have rarely been reported with overdoses less than 7.5 g. In children, amounts less than 150 mg/kg are unlikely to produce hepatotoxicity.
In both adults and children, toxicity associated with acetaminophen is usually caused by ingestion of quantities of the drug that are significantly above the recommended dosage range. Hepatotoxicity, ranging from transient sharp transaminase elevations to fatal, fulminant hepatic failure, is the most common result of clinically significant overdosage29.
In a double-blind, placebo-controlled clinical study, healthy adults were given 4, 6 and 8 g/d of acetaminophen over 3 days30. Plasma concentrations did not accumulate with repeat doses. Clinically all doses were well tolerated by the subjects and aminotransferase values stayed within normal limits throughout the study. These data provide information related to the margin of safety but are not intended to support dosing beyond the maximum recommended dose of 4 g/day.
A report has suggested that hepatotoxicity following greater than the recommended dose of acetaminophen may be enhanced by both prolonged fasting and/or chronic alcohol abuse31.
Acute Alcohol Use
Acute alcohol ingestion refers to the occasional or intermittent use of alcohol. When taken together, alcohol competes with acetaminophen for CYP2E1. CYP2E1 accepts alcohol more readily than acetaminophen; therefore, less NAPQI is produced32. In the presence of alcohol, acetaminophen may be diverted to the glucuronidation and sulfation pathways. The overall result is that a smaller percentage of acetaminophen may be expected to be metabolized to the toxic intermediate, NAPQI, than would otherwise be the case33. NAPQI production is increased above baseline for the period up to 18-24 hours post ethanol clearance from the body. In healthy adults, at normal labeled doses of acetaminophen, the temporary increase in NAPQI production is more than accommodated by normal glutathione stores in the liver.
Hypersensitivity
Sensitivity reactions are rare and may manifest as rash, urticaria, dyspnea, hypotension, laryngeal edema, angioedema, bronchospasm, or anaphylaxis. Cross-reactivity in ASA-sensitive persons has been rarely reported. If sensitivity is suspected, discontinue use of the drug.
Renal Effects
Acute nephrotoxicity has been reported following massive overdose either as a sequela of hepatic failure or, occasionally, in the absence of hepatic failure34.
Clinical data have established that acetaminophen in recommended doses is not nephrotoxic21.
Some studies suggest an association between the chronic long-term use of acetaminophen and renal effects. Results, however, are conflicting, limited by recall bias and confounded by the inability to determine whether analgesic use preceded or followed the onset of renal disease35-40.
Case control studies have suggested a weak association between habitual acetaminophen use and prevalence of chronic renal failure and end stage renal disease12. This National Kidney Foundation position paper concludes that acetaminophen has been preferentially recommended by physicians to patients with renal failure and that there is no evidence that occasional use of acetaminophen caused renal injury. In this position paper, acetaminophen was recommended as the non-narcotic analgesic of choice for episodic use in patients with underlying renal disease.
Special Populations
Pediatric
Lesko and Mitchell41 enrolled more than 84,000 febrile children in a randomized, double blind, acetaminophen-controlled trial to assess the risks of rare but serious adverse events following use of pediatric ibuprofen. Of the children included in the analysis, 28,130 received acetaminophen and none experienced anaphylaxis, or serious hepatic, gastrointestinal or renal effects.
Pregnancy and Lactation
As with any drug, patients who are pregnant or nursing a baby should consult a physician before taking this product.
Pregnancy
Issues of risks in pregnancy are multifactorial. The information provided cannot be substituted for direct patient consultation. Acetaminophen is believed to be non-teratogenic in humans. However, existing studies have not assessed the effect of very high doses. The Motherrisk Collaborative Perinatal project monitored 50,282 motherchild pairs, of which 226 had first trimester exposure to acetaminophen and 781 had used acetaminophen at any time during their pregnancy. No evidence was found to suggest a relationship between acetaminophen use and major or minor malformations42. In a surveillance study of Michigan Medicaid recipients conducted between 1985 and 1992 involving 229,101 completed pregnancies, 9,146 newborns had been exposed to acetaminophen during the first trimester42. This data do not support an association between acetaminophen use and the occurrence of birth defects. Another cohort study, using prescription monitoring, found no excess risk for malformation, and no evidence that acetaminophen influenced fetal growth43. Finally, as part of a larger study, 697 women used acetaminophen with or without codeine in their first trimester. No teratogenic risk was found44.
A prospective study investigated the outcome of pregnancy in 300 women who had selfadministered an overdose of acetaminophen, either alone, or as part of a combined preparation. Exposure to overdose occurred in all trimesters. The majority of the pregnancies had normal outcomes. The malformation rate was within the expected range. There was no obvious relationship between the time of exposure and the time of delivery. The overall conclusion was that acetaminophen overdose is not an indication for termination of pregnancy45.
In a long-term developmental follow-up study46, acetaminophen did not adversely affect IQ or behavior measures at four years of age. Height, weight and head circumference were also not affected by exposure to acetaminophen in-utero.
Unlike ASA, which has been shown to profoundly affect platelet function, there does not seem to be a risk of hemorrhage associated with acetaminophen use at term47,48.
Currently there is no evidence to suggest that acetaminophen is teratogenic when used as recommended. However, data for continuous high daily doses are not sufficient, and safety during pregnancy has not yet been established.
Lactation
Following a typical therapeutic dose, acetaminophen is excreted in breast milk in very low concentrations. Based on a number of published reports49-52, infant exposure levels are at most 4.5% of a weight adjusted pediatric therapeutic dose. In addition, acetaminophen is considered compatible with breast-feeding by the American Academy of Pediatrics53.
Post-Marketing Data
Adverse drug reactions (ADRs) identified during post-marketing experience with paracetamol are included in Table 2. The frequencies are provided according to the following convention: Very common 1/10, Common 1/100 and <1/10, Uncommon 1/1000 and <1/100, Rare 1/10,000 and <1/1,000, Very rare <1/10,000, Not known (cannot be estimated from the available data)
Table 2. Adverse Drug Reactions Identified during Post-Marketing Experience with Therapeutic Doses of Acetaminophen by Frequency Category Estimated from Spontaneous Reporting Rates:
| System Organ Classification Frequency | Adverse Event Preferred Term |
|---|---|
| Investigations | |
| Very rare | Transaminases increased† |
| Immune System Disorders | |
| Very rare | Anaphylactic reaction |
| Very rare | Hypersensitivity |
| Skin and Subcutaneous Tissue Disorders | |
| Very rare | Fixed eruption |
| Very rare | Urticaria |
| Very rare | Pruritic rash |
| Very rare | Rash |
† Low level transaminase elevations may occur in some patients taking labeled doses of acetaminophen; these elevations are not accompanied with liver failure and usually resolve with continued therapy or discontinuation of acetaminophen.
Drug interactions
Analgesics
Caution is recommended when analgesic products are used in combination because of possible increases in adverse events (e.g. nephrotoxicity, gastrointestinal lesions, bleeding).
Alcohol
Studies evaluating the metabolism of doses up to 20 mg/kg of acetaminophen in chronic alcohol abusers and a study evaluating the effects of 2 days of acetaminophen dosing at 4000 mg/d in chronic alcoholics undergoing detoxification, have yielded inconsistent results with regard to effects on acetaminophen pharmacokinetics and demonstrate no evidence of adverse effect on liver function tests3-6,54,55.
Anticoagulants - Oral
Patients who concomitantly medicate with warfarin-type anticoagulants and regular doses of acetaminophen have occasionally been reported to have unforeseen elevations in their INR. Physicians should be cognizant of this potential interaction and monitor the INR in such patients closely while therapy is established. Many factors, including diet, medications, and environmental and physical states, may affect how a patient responds to anticoagulant therapy56. There have been several reports that suggest that acetaminophen may produce hypoprothrombinemia (elevated international normalized ratio [INR] or prothrombin time) when administered with coumarin derivatives57-59. In other studies, prothrombin time did not change60-62. Reported changes have been generally of limited clinical significance, however, periodic evaluation of prothrombin time should be performed when these agents are administered concurrently.
In the period immediately following discharge from the hospital or whenever other medications are initiated, discontinued, or taken regularly, it is important to monitor patient response to anticoagulation therapy with additional prothrombin time or INR determinations56. Despite the potential for interaction, acetaminophen is the least likely OTC analgesic to interfere with anticoagulant therapy and thereby remains the OTC analgesic of choice for concomitant use.
Patients should be instructed to ask a physician or pharmacist before use if they are taking the blood thinning drug warfarin or other coumarin derivatives.
Anticonvulsants
Some reports have suggested that patients taking long-term anticonvulsants, who overdose on acetaminophen, may be at increased risk of hepatotoxicity because of accelerated metabolism of acetaminophen63,64. Available data are conflicting. A 7-year retrospective study of acetaminophen overdose admissions indicates that the overall mortality rate was not significantly different for patients taking concomitant anticonvulsant medications65.
Hydantoins
At usual oral therapeutic doses of acetaminophen and hydantoins, no special dosage adjustment or monitoring is generally required. Pharmacokinetic studies indicate that phenytoin primarily induces the glucuronidation pathway, whereas glutathione-derived metabolites are not increased in patients on chronic phenytoin therapy66. Additionally, recent data demonstrate that phenytoin is metabolized primarily by CYP2C9 and CYP2C1967, whereas acetaminophen is primarily metabolized by CYP2E168. These data indicate that there is no increased risk of acetaminophen hepatotoxicity in patients on chronic hydantoin therapy who use the recommended dose of acetaminophen.
Carbamazepine
At usual oral therapeutic doses of acetaminophen and carbamazepine, no special dosage adjustment is generally required. Carbamazepine is primarily metabolized by CYP3A467, whereas acetaminophen is metabolized primarily via CYP2E1. It is not known whether there is increased risk from an acetaminophen overdose in patients on chronic carbamazepine therapy.
Diflunisal
Professional literature from the manufacturer of diflunisal cautions that concomitant administration with acetaminophen produces an approximate 50% increase in plasma levels of acetaminophen in normal volunteers56. Acetaminophen had no effect on diflunisal plasma levels. The clinical significance of these findings has not been established. However, caution should be used with concomitant administration of diflunisal and acetaminophen and patients should be monitored carefully.
Isoniazid
Some reports suggest that patients on chronic isoniazid therapy may be at risk for developing hepatotoxicity from an acetaminophen overdose69-71. Since patients on isoniazid therapy may develop hepatic effects from isoniazid alone, data from individual case reports are unclear as to whether chronic administration of isoniazid may increase the risk of acetaminophen toxicity. Isoniazid is primarily metabolized by CYP2E172,73 and induces CYP2E163,72,74,75. Studies in healthy subjects demonstrate that isoniazid blocks the formation of the toxic metabolite NAPQI when administered concomitantly with acetaminophen, but increase NAPQI formation when acetaminophen is administered one day after discontinuation of isoniazid76,77. Thus, concomitant use of isoniazid is unlikely to potentiate the risk of acetaminophen-induced hepatotoxicity at recommended doses. The isoniazid induction of CYP2E1 is short-lived, lasting only 12 to 48 hours after the discontinuation of isoniazid77,78; it is during this period the toxicity of an acetaminophen overdose may be potentiated.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.