BETAPYN Tablet Ref.[51189] Active ingredients: Caffeine Codeine Doxylamine Paracetamol
Source: Health Products Regulatory Authority (ZA) Revision Year: 2021 Publisher: Adcock Ingram Limited, 1 New Road, Erand Gardens, Midrand, 1685
4.1. Therapeutic indications
For the symptomatic treatment of mild to moderate pain and/or fever.
4.2. Posology and method of administration
Posology
Adults and children over 12 years: 1 or 2 tablets taken orally, repeated 4-hourly if necessary. Do not exceed 8 tablets per day.
DO NOT EXCEED THE RECOMMENDED DOSE.
4.9. Overdose
Prompt treatment is essential. In the event of an overdosage, consult a doctor immediately, or take the person directly to a hospital. A delay in starting treatment may mean that antidote is given too late to be effective. Evidence of liver damage is often delayed until after the time for effective treatment has lapsed.
Susceptibility to paracetamol toxicity is increased in patients who have taken repeated high doses (greater than 5-10 g/day) of paracetamol for several days, in chronic alcoholism, chronic liver disease, AIDS, malnutrition, and with the use of drugs that induce liver microsomal oxidation such as barbiturates, isoniazid, rifampicin, phenytoin and carbamazepine. Symptoms of paracetamol overdosage in the first 24 hours include pallor, nausea, vomiting, anorexia and possibly abdominal pain. Mild symptoms during the first two days of acute poisoning, do not reflect the potential seriousness of the overdosage.
Liver damage may become apparent 12 to 48 hours, or later after ingestion, initially by elevation of the serum transaminase and lactic dehydrogenase activity, increased serum bilirubin concentration and prolongation of the prothrombin time. Liver damage may lead to encephalopathy, coma and death.
Acute renal failure with acute tubular necrosis may develop even in the absence of severe liver damage. Abnormalities of glucose metabolism and metabolic acidosis may occur. Cardiac arrhythmias have been reported.
Treatment for paracetamol overdosage
Although evidence is limited it is recommended that any adult person who has ingested 5-10 grams or more of paracetamol (or a child who has had more than 140 mg/kg) within the preceding four hours, should have the stomach emptied by lavage (emesis may be adequate for children) and a single dose of 50 g activated charcoal given via the lavage tube. Ingestion of amounts of paracetamol smaller than this may require treatment in patients susceptible to paracetamol poisoning (see above). In patients who are stuperose or comatose endotracheal intubation should precede gastric lavage in order to avoid aspiration.
N-acetylcysteine should be administered to all cases of suspected overdose as soon as possible preferably within eight hours of overdosage, although treatment up to 36 hours after ingestion may still be of benefit, especially if more than 150 mg/kg of paracetamol was taken. An initial dose of 150 mg/kg N-acetylcysteine in 200 ml dextrose injection given intravenously over 15 minutes, followed by an infusion of 50 mg/kg in 500 ml dextrose injection over the next four hours, and then 100 mg/kg in 1 000 ml dextrose injection over the next sixteen hours. The volume of intravenous fluid should be modified for children.
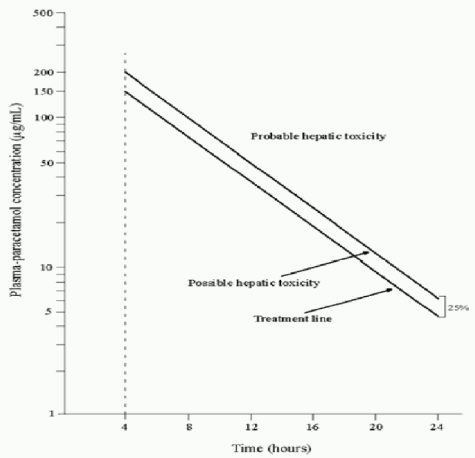
Although the oral formulation is not the treatment of choice, 140 mg/kg dissolved in water may be administered initially, followed by 70 mg/kg every four hours for seventeen doses. A plasma paracetamol level should be determined four hours after ingestion in all cases of suspected overdosage. Levels done before four hours may be misleading. Patients at risk of liver damage, and hence requiring continued treatment with N-acetylcysteine, can be identified according to their 4-hour plasma paracetamol level. The plasma paracetamol level can be plotted against time since ingestion in the nomogram below. The nomogram should be used only in relation to a single acute ingestion.
Those whose plasma paracetamol levels are above the "normal treatment line", should continue N-acetylcysteine treatment with 100 mg/kg IV over sixteen hours repeatedly until recovery. Patients with increased susceptibility to liver damage as identified above, should continue treatment if concentrations are above the "high risk treatment line". Prothrombin index correlates best with survival.
(Reference: Martindale 37th Edition)
Codeine phosphate: Symptoms of overdosage with codeine include excitement and in children, convulsions may occur. Treatment is symptomatic and supportive.
Doxylamine succinate: The most common symptom of overdosage is impaired consciousness and additionally psychotic behaviour.
Caffeine: Overdose may cause diuresis, tachycardia, irritability, nervousness, restlessness, gastrointestinal disturbances and CNS stimulation such as agitation, excitement, insomnia and tremors. The management of caffeine toxicity is generally symptomatic and supportive (e.g., hydration). For acute ingestion gastric lavage is advised.
6.3. Shelf life
24 months.
6.4. Special precautions for storage
Store at or below 30°C in a cool, dry place.
Do not remove the blister pack from the outer carton until required for use.
Store in a safe place, out of reach of children.
6.5. Nature and contents of container
PVC/Aluminium foil blister packs of 18, 20 and 40 tablets.
All pack sizes may not be marketed simultaneously.
6.6. Special precautions for disposal and other handling
No special requirements.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.